Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124


 Access video and video lecture content for this chapter online at Elsevier eBooks+
Access video and video lecture content for this chapter online at Elsevier eBooks+
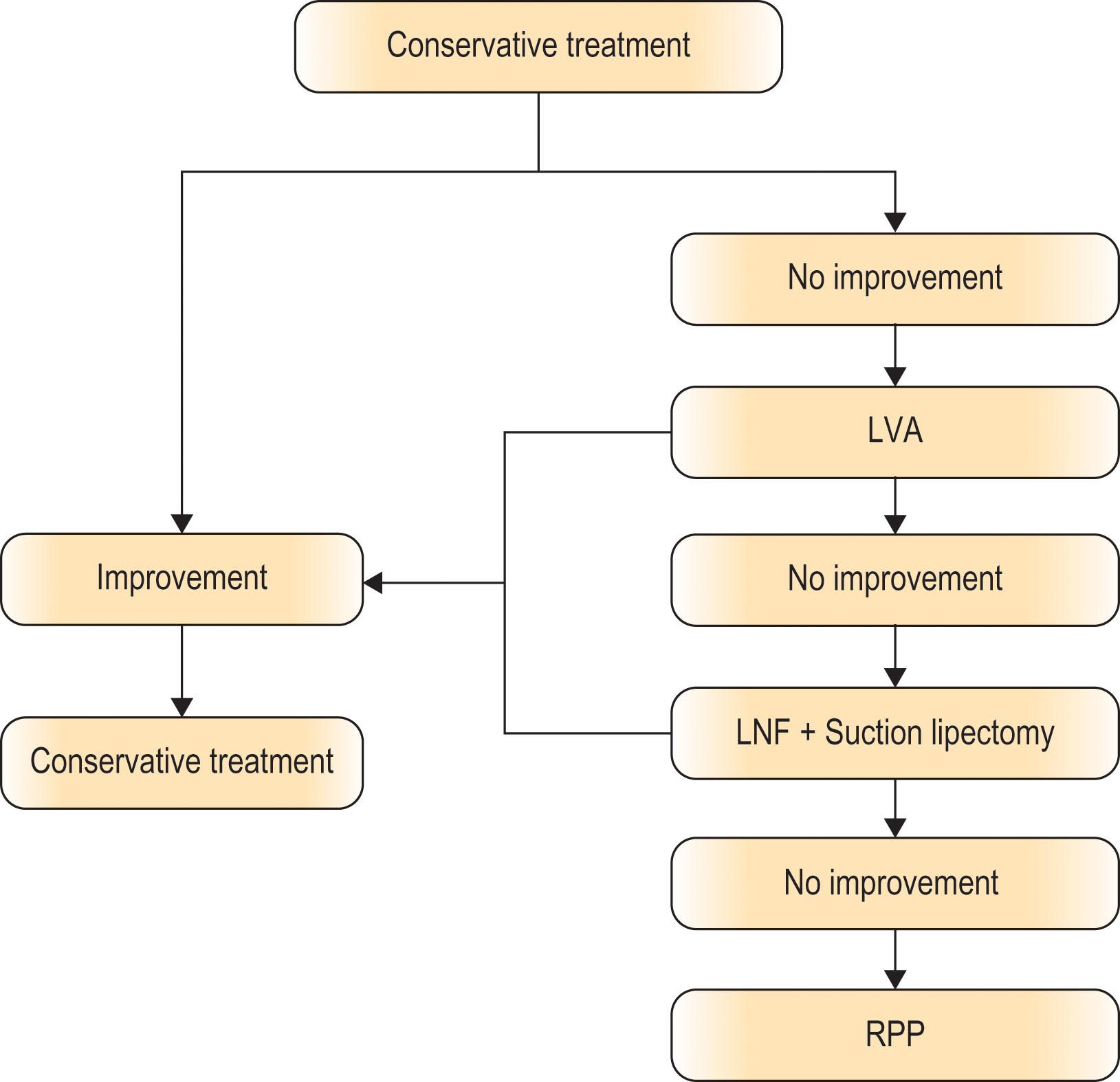
In advanced lymphedema, chronic inflammation and repeated episodes of infection lead to gradual fibrosis of subcutaneous tissue and skin, causing destruction of lymphatic channels, and it is not suitable for microsurgical lymphovenous anastomosis. The most important goal of treatment for lymphedema is control or eradication of infection. In particular, prevention of toe infection has proven to be an important step in controlling cellulitis of the lower limb. Historically, the Charles procedure was first described in 1940. The Charles procedure was a common treatment to decrease lymphatic load and to control infection. Patients with primary or secondary advanced lower limb lymphedema with induration, fibrosis, brawny leather-like skin, “squared-off” toes, hyperkeratosis, and multiple fistulas can be treated with the Charles procedure. Potential complications of the Charles procedure are wound breakdown, hyperkeratosis, ulceration, and aggravation of foot lymphedema. To prevent these problems, many authors have described a modified Charles procedure. Van der Walt et al . presented a modified Charles procedure, applying negative-dressing after the initial debulking surgery, and then they delayed the skin grafting by 5–7 days. The excisional procedure may be simultaneously performed with toe amputations. The excisional procedure can be combined with lymph node flap transfer, as in the Chen-modified Charles procedure, in which 10 steps are different from the original Charles procedure.
An important anatomic detail is that the Chen-modified Charles procedure consists of preserving the lesser saphenous vein along with its superficial branch. The excisional procedure can be combined with lymphatic microsurgery. A circumferential incision is marked with two wedge incisions on the proximal thigh, one on the medial aspect and the other on the lateral. Distally at the foot and toes, markings are placed at the mid-lateral and medial aspect of the foot, above the heel, and on the dorsum of the toes and web spaces, preserving the web spaces between the toes. The treatment of toes depends on different severity of toe involvement.
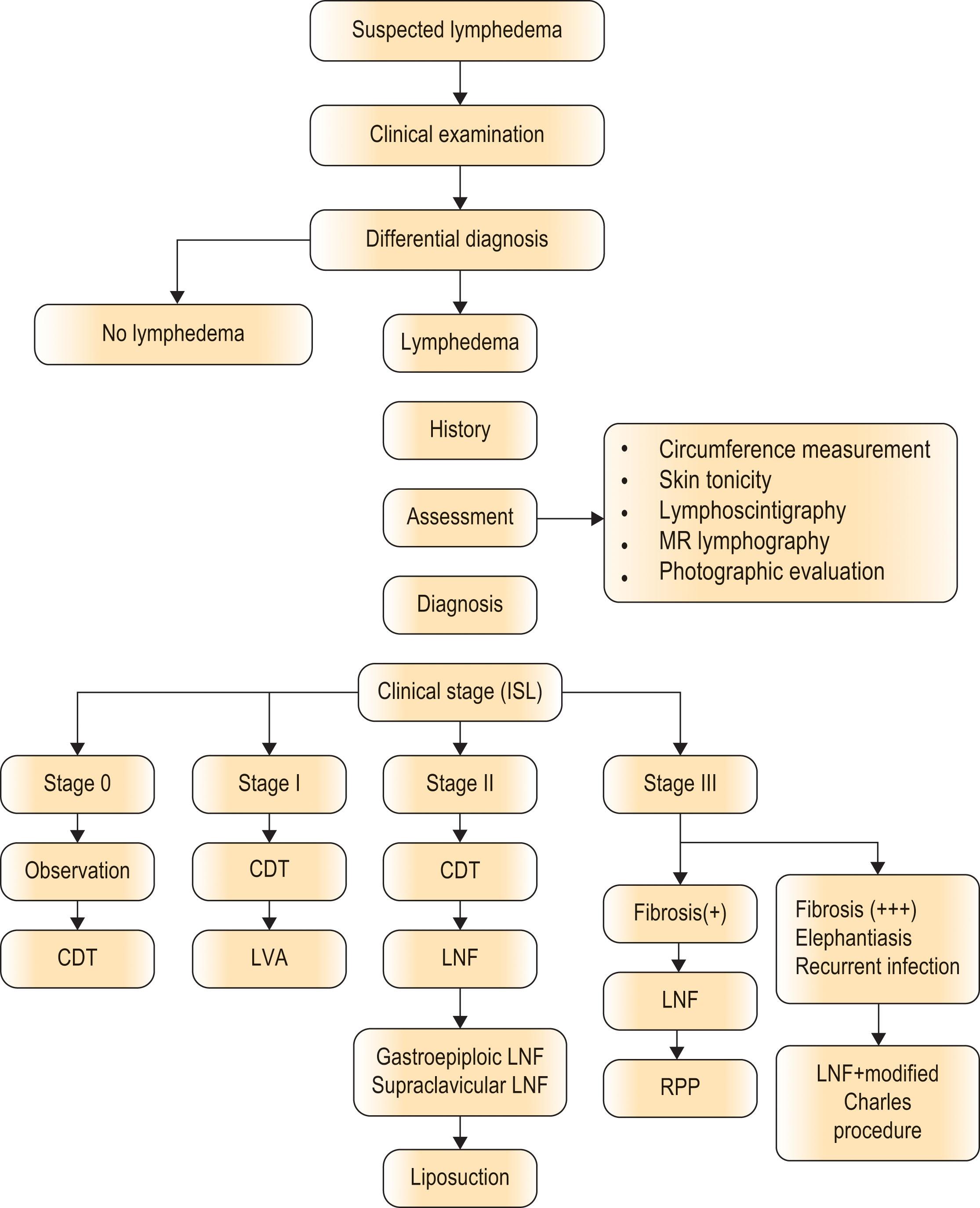
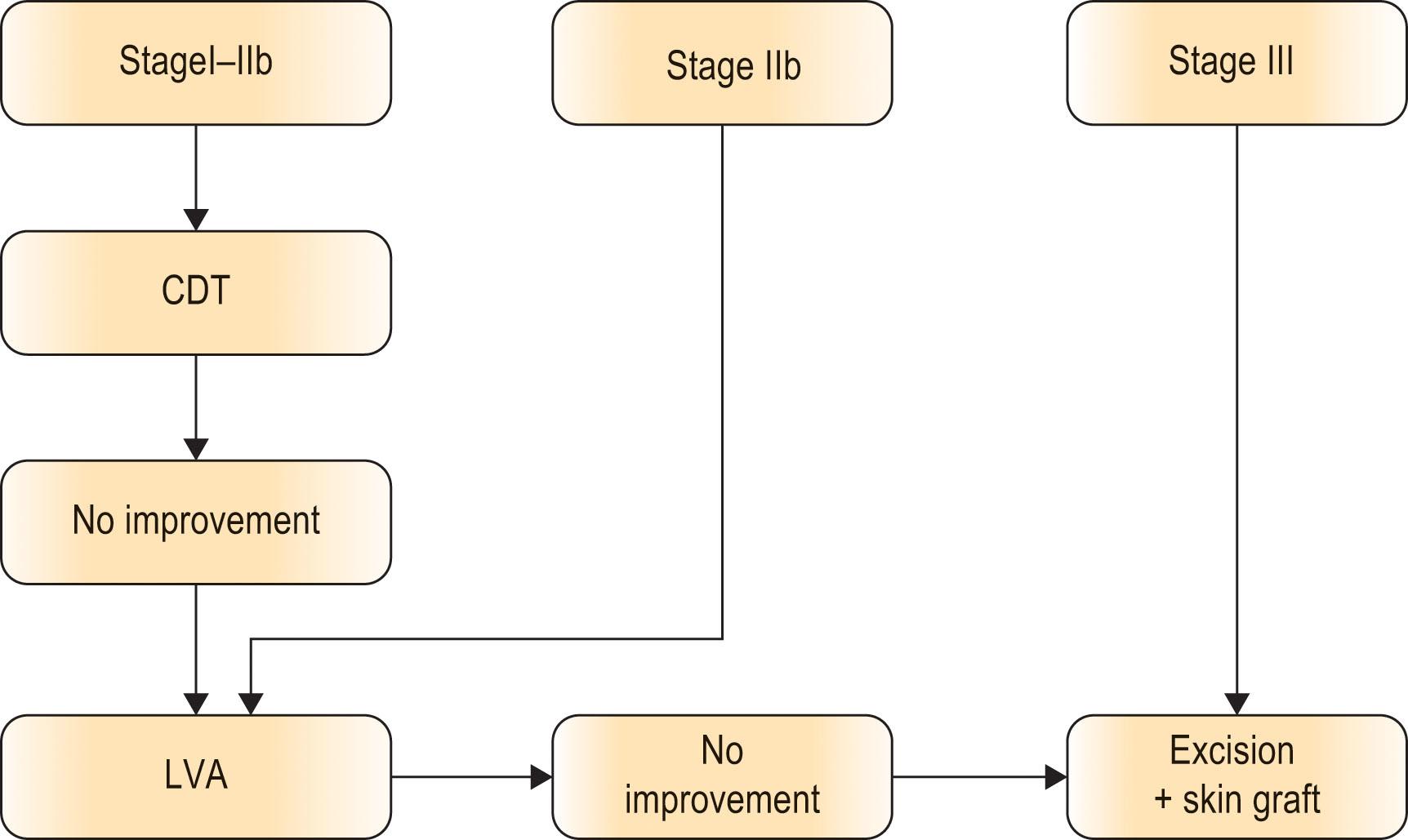
The International Society of Lymphology divides the severity of lymphedema into three stages. Karri et al . reported a modified staging system, dividing the severity of the pathology into four stages. According to their system, advanced lymphedema is characterized by irreversible skin fibrosis (IIIb); and non-pitting edema, with leather-like skin, skin crypts, and ulcer, without or with involvement of the toes (stage IVa and IVb, respectively). In advanced lymphedema, the most important goal of treatment is control or eradication of infection. Toes are the major source of infection, especially in older patients. Toe crowding, nail infections, skin changes such as verrucous hyperkeratosis, and poor hygiene can all contribute to infection of toes, which may ascend to the foot or even proximal leg. If the toes are affected but left untreated, the patient will invariably have recurrent infections with a compromised result.
On hospital admission, the circumference of the affected limb is measured by a plastic surgery specialist nurse. Measurements are taken at four levels: midfoot, ankle (between medial and lateral malleoli), mid-calf (15 cm below knee joint), and mid-thigh (15 cm above knee joint). Routine preoperative investigations are performed and anesthetic consultation is provided. Antibiotics are given according to bacterial culture one hour before induction and continued postoperatively for three days.
 Good exsanguination is very important to minimize blood loss. The patient may lose a significant amount of blood if the bleeding is not well controlled. (B) The area of excision for the indurated skin and subcutaneous tissue is very large. However, we should still be patient to do it carefully. This is a very laborious procedure, and multiple plastic surgeons are required for the procedure of excision and hemostasis. (C) This picture shows the very large area of excision in the modified Charles procedure. (D) Advanced lymphedema was due to repetitive occurrences of infection. The skin was very thick and fibrotic, like leather. The subcutaneous tissue was also as hard as rock, which could not be removed with suction lipectomy. Also, LVA would not work for this patient. (E) Intraoperative picture after the modified Charles procedure. The strips of split skin graft were arranged in a circular manner. (F) Full-thickness skin graft was put over the dorsum of the foot to prevent future ulcer due to frequent friction with the compression garment.")
The patient is positioned supine, and a pneumatic tourniquet is placed on the proximal thigh and inflated to 375 mmHg following exsanguination. Split-thickness skin graft (STSG) is harvested from the entire circumference of the affected limb in a proximal to distal (axial) direction with the thickness of 12/1000 of an inch. It is imperative that the lengths of the harvested STSG are as long as possible. The STSG can thus be “wrapped” around the limb in a circular fashion. Consequently, the risk of hypertrophic scar formation is minimized. The harvested STSG sheets are fenestrated. The leg is denuded down to the deep fascia. To access the posterior surface of the limb, a 3-mm K-pin is drilled through the distal tibia and the limb is suspended from a stand. This pin can also help to elevate the leg after surgery and is usually removed five days postoperatively at bedside. The fibrosclerotic lymphedematous tissue is then separated from the deep fascia using blunt and sharp dissection. The thickened deep fascia is also trimmed to its normal size. Toes are amputated if there are recurrent infections, verrucous hyperkeratosis, or osteomyelitis. Otherwise, nails and nail beds are removed, and the defect is closed using C–V or rotation advancement flaps, to preserve toe length. The tip of the distal phalanx of the toe can be shortened by 0.5 cm if there is any tension during wound closure. The procedure of excision and control of the major bleeders should be completed within two hours of tourniquet ischemia time. Therefore, a team of surgeons is necessary. While waiting for hemostasis, the proximal thigh can be debulked. Two wedge excisions are made starting at the medial and lateral mid-axial lines. The resultant soft tissue on anterior and posterior thigh flaps is thinned tangentially to 2 cm and sutured together to the deep fascia to allow a smoother transition from the distal grafted thigh to the skin flaps of proximal thigh. Suction drains are left in situ . A full-thickness skin graft (FTSG) is taken from the wedge-excised tissues and is used for grafting at the dorsum of the foot. (FTSG on the dorsum of the foot results in a more resistant skin graft with less hypertrophic scarring and can prevent later friction with the compression garment.) The tourniquet is re-inflated, and the split-thickness skin graft is applied circumferentially with 0.5–1 cm edge overlap to prevent gap formation between the sheets of skin grafts, which may arise because of swelling. This is aimed at minimizing the formation of hypertrophic scar. Finally, nonadherent dressings, bulky gauze, compression wrap, and a posterior splint are applied. The tourniquet is then deflated. Elevation of the limb and thus avoidance of shearing force ensures STSG take on the posterior surface of the leg and thigh.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here