Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

This chapter will help illustrate the ease with which virtual surgery and computer-aided design and manufacturing can be used to create accurate postoperative results and provide confidence with complex three-dimensional bony injuries and reconstructions.
With advancements in software technology and three-dimensional printing, our ability to plan and execute precise bony reconstruction has become a reality.
With this technology, guides can be made to ensure exact bony repositioning and replacement. These personalized surgical devices can help guide precise bone cutting at the donor and recipient sites, anywhere in the body, and facilitate precise positioning and apposition of bone for any type of reconstruction.
With use of these computer-aided design tools, along with the addition of guidance technology, the position of the bone can be guaranteed intra-operatively.
We review our method in approaching some of these problems and illustrate the application of these techniques for mandibular reconstruction, maxillary reconstruction, maxillofacial trauma, frontal sinus reconstruction, and temporomandibular joint reconstruction. This technology continues to evolve, and our indications for its application continue to grow. This chapter represents only a small portion of the types of cases in which these techniques can be applied.
Craniofacial, maxillofacial, and head and neck ablative surgery existed long before the field of head and neck reconstruction was recognized as a sub-specialty. This historical lack of head and neck reconstruction severely limited the surgeon’s ability to perform any type of complex head and neck ablative, trauma, and congenital surgery. Advances first in pedicled flap surgery and then in microsurgery techniques forever changed the field of head and neck surgery. The ability now to reconstruct larger and larger composite defects provided increased freedom to the ablative surgeon.
Similarly, over the last generation, improvements made in imaging technology have been a major advance for the reconstructive surgeon. Radiographic techniques such as computed tomography (CT) imaging have allowed the surgeon to assess a defect or injury and helped them to plan a more precise and strategic reconstruction. New approaches and operative techniques were developed because of these advances. However, even with this initial advancement in imaging technology, the surgeon still only had a two-dimensional representation of a three-dimensional problem. There was no physical translation that could be made between the images and the patient. The information obtained from imaging was best translated through anatomic knowledge and increased experience from the surgeon.
When repairing the three-dimensional bony architecture of the craniofacial skeleton, one is visually limited by access and the inability to gain complete three-dimensional exposure of the desired surgical sites. Also, because of the three-dimensional nature of the craniofacial skeleton, even small degrees of error can lead to poor outcomes. Traditional reconstructive techniques require a large learning curve and teaching of these techniques can be difficult, leading to inconsistent results, especially with less experienced surgeons. Surgical experience and an innate sense of three-dimensional anatomy have been required historically to obtain optimum outcomes. However, not all surgeons have the same skill set or experience so outcomes inevitably have been more variable.
With advances made over the last decade in computer modeling and virtual surgery, we are now able to translate the information received from radiographic imaging studies to actual intra-operative tools that can help us overcome the complex three-dimensional anatomy of the head and neck ( Fig. 6.3.1 ). This has led to more predictable and more functional outcomes for the patient. Use of these techniques also allows a less experienced surgeon the potential to obtain similar outcomes to a more experienced one. As these techniques improve and are utilized along with guidance technology, accuracy and surgical outcomes will continue to be maximized.
When planning a resection, the CT scan should be relatively close in time to the planning session and the surgery. The modeling team should outline the tumor and generous margins should be planned. It is best to do this with the ablative team directly so that they agree with this plan. If there is a question about margin safety and need for further intra-operative resection, an alternate guide can be made to accommodate for these potential changes intra-operatively.
Take into account soft-tissue needs when planning these procedures. Take as much skin as you need from your primary flap or consider alternative secondary flaps if a complex resection is planned and there is a large intra- and extra-oral soft-tissue requirement.
In cases with significant tissue loss or lack of tissue flexibility, such as in radiation injury, the bony reconstruction can be designed to minimize the strain on the remaining soft tissues, decreasing the complexity of the reconstruction.
All specialties involved in the surgical and perioperative treatment should be invited and should try to attend the virtual planning session. The involvement of the entire team will allow for fewer critical errors in the planning process. Also, each team should evaluate the plan that is created by the engineers after this meeting and sign off before the plans are considered final.
As the reconstruction becomes more complex with multiple bony segments, predesigned plates can play an important role in obtaining very precise reconstruction results.
Consider primary osseointegrated implants in benign cases or in select oncologic cases.
When designing the reconstruction, plan for bone segments to remain at least 2 cm in length to maintain appropriate circulation.
Use virtual planning to position appropriately the bone segments. With appropriate imaging, perforators can be noted preoperatively, which assist in the soft-tissue design. For fibula flap harvest, make sure to maintain a sufficient proximal and distal osteotomy so that knee and ankle stability is not affected.
When bone loss or malposition is part of the deformity, first reposition the bone with the assistance of imaging technology, prior to planning any flaps or grafts that might need to be used. This can be achieved using mirror-imaging techniques of the contralateral unaffected side.
When using multisegmental repositioning or complex rotational segments where alignment is critical, such as in implant placement, make intermediary splint devices to help confirm the position of the reconstruction while advancing through each step.
 A stereolithographic model of the skull with the tumor and virtual cuts colored. (B) The cutting guide specific to the patient’s fibula and mandible are noted along with an occlusal splint.")
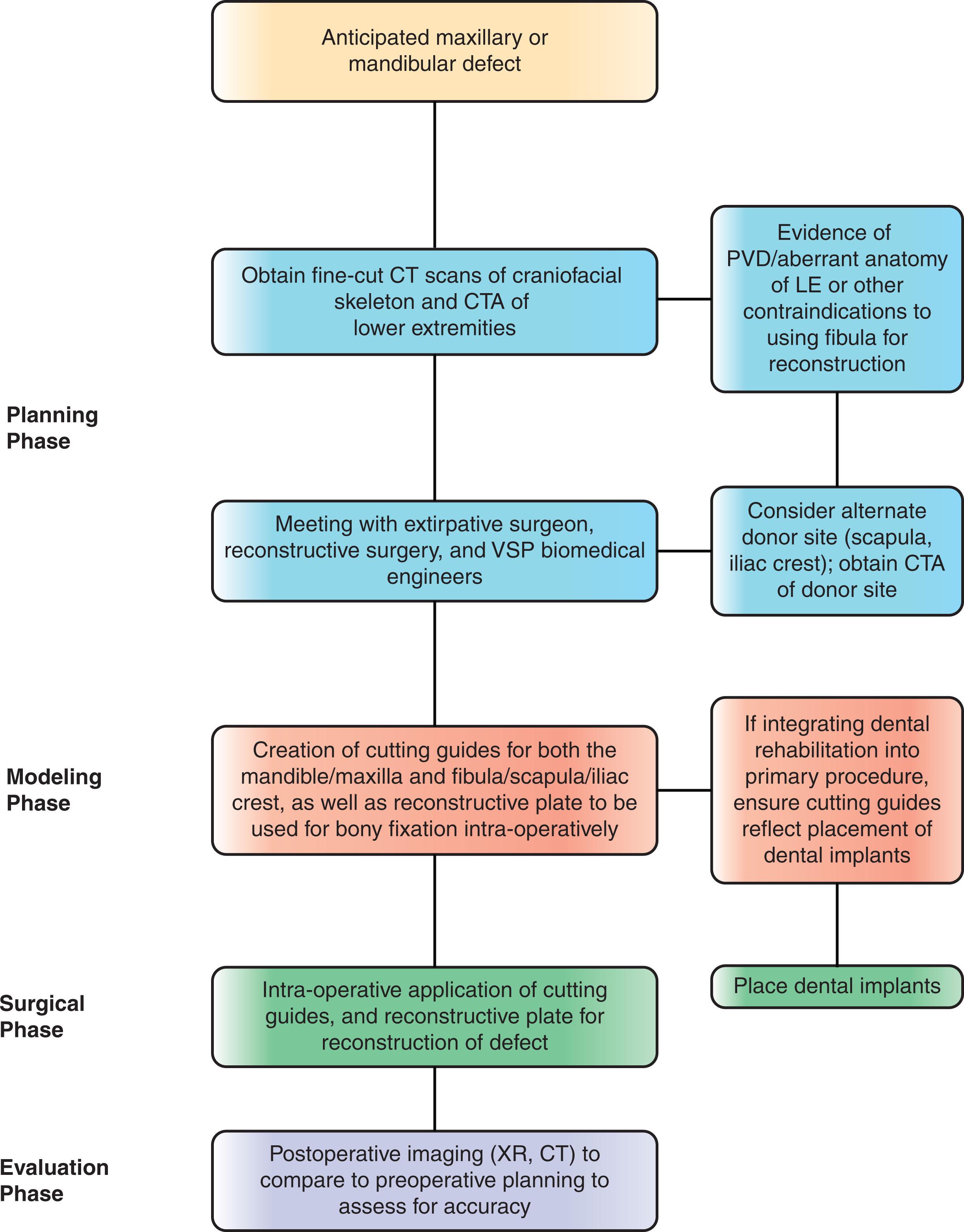
At our institution, we have utilized three-dimensional facial analysis and virtual surgical planning (VSP) in all of our craniomaxillofacial reconstructive and ablative cases. Over the past thirteen years, many cases have been planned, modeled, and executed in this manner and have led to more reliable and predictable outcomes ( Algorithm 6.3.1 ). Over this time period we have continuously refined these techniques, and this approach has revolutionized the way we diagnose, treat, and reconstruct head and neck diseases and defects. In all aspects of surgery, proper planning facilitates more predictable operative results, but prior to the use of VSP, much of this relied on two-dimensional imaging and surgical trial and error. It has been our goal to make all forms of reconstructive surgical procedures, including oncologic, traumatic, congenital, and aesthetic, treatable with this methodology. These techniques are teachable, have a shallow learning curve, allow for precise and anatomic bony reconstruction and ultimately decrease surgical time. In specific cases, we have married VSP with navigation guidance technology to allow for even more accuracy in both ablative and reconstructive procedures when indicated ( Fig. 6.3.2 ).

The goal of this chapter is to illustrate how virtual surgery and computer-assisted design can be utilized by the surgeon to decrease operative time and create accurate postoperative results compared to traditional craniomaxillofacial surgical treatment planning. We will review our methodology in approaching some of these problems and illustrate application of these techniques. This will only be a small representation of the types of cases where we have applied VSP, and we feel the applications will continue to broaden as surgeons discover the ease in which their operations can be planned and executed. We have reliably achieved excellent results in both malignant and benign head and neck oncologic surgery and reconstruction, orthognathic surgery, maxillofacial trauma, temporomandibular joint reconstruction, and skull base surgery. These techniques have become our preferred method for complex craniomaxillofacial surgery and reconstruction.
The evolution of our current technique began with the use of stereolithographic models as templates ( Fig. 6.3.3 ). These models were printed directly from the CT scan and were used preoperatively to bend plates around the presumed bony resection and/or to develop plates to work around exophytic lesions. Intra-operatively, these models were used for reference to help us navigate these operations. We first utilized this technique and these models for mandibular reconstruction after tumor resection. This was an area where we felt there was great variability in outcomes based on how well all the bony segments were reconstructed. Although helpful, this approach was still quite labor intensive and there was still often “guesswork” and room for error in performing osteotomies of the mandible and fibula correctly, aligning the released jaw segments, and insetting the fibula into the resection site. Our technique has evolved to involve pre-planning each phase of the operation, including the osteotomies on the mandible and the lower extremity by using staged cutting guides and prefabricated plates, which allows for surgically efficient and highly predictable outcomes as far as bone and soft-tissue positioning. We continue to refine cutting guide design and surgical planning to include placement of permanent implants and dentures. We will describe the basic process of planning and using computer-aided design/computer-aided manufacturing (CAD/CAM) technology for reconstruction.

Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here