Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Access video lecture content for this chapter online at Elsevier eBooks+ 
The treatment of breast cancer is constantly evolving. Surgery remains an important pillar, but the use of radiotherapy (RT) has increased dramatically due to its clinical benefit in reducing risk of locoregional recurrence and improving the overall survival rate in high-risk patients. Despite the oncological benefits of RT, most patients will experience adverse effects in the treated area that may contribute to tissue changes over a prolonged period of time. This represents a significant challenge for the reconstructive surgeon when considering the most reliable and esthetically-viable breast reconstruction (BR) technique. The three most likely scenarios are: (1) BR in the context of breast-conserving surgery and RT; (2) BR in the setting of postmastectomy radiotherapy (PMRT); and (3) BR in a pre-irradiated field. This chapter describes current considerations on RT in the treatment of breast cancer and its effects on tissues and reviews the various BR procedures available for each potential scenario.
In recent years, RT in breast cancer treatment has changed enormously, in terms of the indications after conservative or radical breast surgery, as well as the criteria for irradiation of regional lymph node areas. The main improvements include the development of new technologies, quality controls, radiation dose, and fractionation schedules.
Since the early twentieth century, RT has been used as an adjuvant treatment in breast cancer. The oldest methods, such as radium needles or orthovoltage units, were flawed by poor understanding of how to fractionate and deliver the total radiation dose to the target volumes. For several decades, cobalt-60 sources were also used in treatment, but in the 1980s the widespread use of linear accelerators employing 4-10 megavolt beams improved beam homogeneity and dose calculation for better quality control of irradiation. Further improvements included therapy via multi-leaf collimators, intensity-modulated RT, image-guided RT, which allows accurate verification and quality control ( Fig. 48.1 ), and respiratory-gated radiotherapy, which uses a deep inspiration breath-hold technique. In the last 20 years, new irradiation devices have been designed. These include tomotherapy, which combines an accelerator and an image-control device on a ring, delivering very precise treatments. Huge, expensive, proton accelerators are also used to treat some breast cancers when there is complex anatomy or target volumes, allowing even better dose distribution. Intraoperative partial breast irradiation involves a less complex procedure using mobile electron linear accelerators or miniature units of low energy photons (50 kilovolts).
 and image-guided RT.")
The traditional dose used for local and/or regional adjuvant therapy is 45–50 gray (Gy), in 25–28 fractions of 1.8–2.0 Gy. However, evidence published in the Canadian and UK START trials has shown similar efficacy and comparable side effects with shorter fractionation schedules. Thus, moderate hypofractionation is currently the standard schedule, consisting of 13–16 fractions with an individual dose of 2.66–3 Gy, up to a total dose of approximately 39–45.5 Gy. In some cases, a radiation boost may be recommended at the end of treatment. This is a supplementary 10–16-Gy dose of radiation administered in 2-Gy fractions, aimed directly at the area from where the cancer was surgically removed. However, higher dose-per-fraction schedules are being used to treat small amounts of breast tissue (partial breast irradiation) in well-selected patients with low risk of relapse. In 2020, the long-term outcome data of a 1-week schedule of 26 Gy in five fractions (FAST-Forward trial) was also reported, showing it to be effective and safe with milder early skin reaction.
After conservative breast surgery, almost all patients have an indication for postoperative irradiation, but omission of adjuvant RT is the subject of study in several ongoing trials. In most cases, whole breast irradiation is recommended, and the target volume includes all breast tissue outside the pectoral fascia. The external radiation is delivered using tangential beams or combined dynamic arc techniques and intensity-modulated RT. For well-selected patients with low-risk tumor features, partial breast irradiation can be delivered through external or internal radiation. Internal radiation includes several techniques such as brachytherapy, balloon implants, or intraoperative devices. The choice will depend on the position, size and type of cancer and technique availability. For tumor bed boosts it is encouraged to mark the surgical bed with clips to ensure the correct dose at the right level. Preoperative irradiation is being investigated as an alternative, with the intention of reducing tumor size prior to surgery, allowing a more localized resection. This could favor the immediate reconstruction of defects.
PMRT is a well-established component in the treatment of breast cancer in patients with locally-advanced disease. In T2 tumors, PMRT may also be considered in young patients or those with unfavorable pathologic findings. If lymph nodes are involved, PMRT is always indicated independently of tumor size because of the risk of spread via subcutaneous lymph vessels. After axillary lymph node dissection, level 3 and 4 are included in the RT. RT to all four levels is also recommended after positive sentinel lymph node biopsy without subsequent lymph node dissection. Irradiation to the internal mammary chain can be considered according to tumor size, location in the breast, age, and risk factors.
Typically, old-fashioned technology usage was accompanied by high toxicity to the breast, lung, heart, and chest tissues, compromising treatment tolerance and survival outcomes. Recent improvements in radiation physics, computer technology and calculation software have allowed better distribution and higher-quality administration of doses ( Fig. 48.2 ). Nevertheless, irradiation of healthy tissues cannot be avoided entirely. The side effects of RT on tissues are produced by a biphasic process divided into immediate and delayed. Acute side effects that appear during or soon after RT administration are a consequence of the altered cell turnover cycle in rapidly proliferating cells, resulting in cell death. Early lesions include generalized edema, skin erythema, hyperpigmentation, and ulceration, which can range from mild to severe. Usually, these initial reactions are transient and resolve with appropriate care measures. However, chronic changes secondary to the inflammatory response can occur, posing the need for cautious monitoring during treatment and follow-up. Delayed skin toxicity involves telangiectasia, dyspigmentation, dyschromia, dryness, and skin atrophy. Clinically, the replacement of normal adipose tissue by collagen causes hardening and thickening of the dermis and compromises tissue microcirculation. These changes may occur several months after radiotherapy, but can take years to fully manifest. In addition, fibrosis and shrinkage of the breast can occur. These late effects are the main factors responsible for interfering with breast reconstructive surgery.

Breast-conserving surgery together with RT has become the mainstay of treatment of early-stage breast cancer. However, tumor removal leaves a postsurgical deformity that can have a major effect on cosmesis. In addition, side effects of adjuvant RT can alter the condition the operated breast, making the aesthetic outcome even more unpredictable and frequently unsatisfactory. In this context, an oncoplastic approach has gained universal acceptance because it allows the surgeon to perform wider local excisions for optimal cancer control and repair the defect to minimize the risk of deformity or asymmetry between breasts.
The techniques to repair the defect after breast-conserving surgery can be classified into two types: (1) Volume displacement procedures , in which breast parenchyma is reorganized to repair the defect: these techniques include different types of local breast tissue rearrangement, mastopexy, and reduction mammoplasty ; (2) Volume replacement procedures , where nearby tissue is recruited to fill in the defect: these techniques involve local perforator flaps that can be based on the thoracodorsal or lateral thoracic artery perforators (TDAP and LTAP), as well as lateral, medial or anterior intercostal artery perforators (LICAP, MICAP and AICAP).
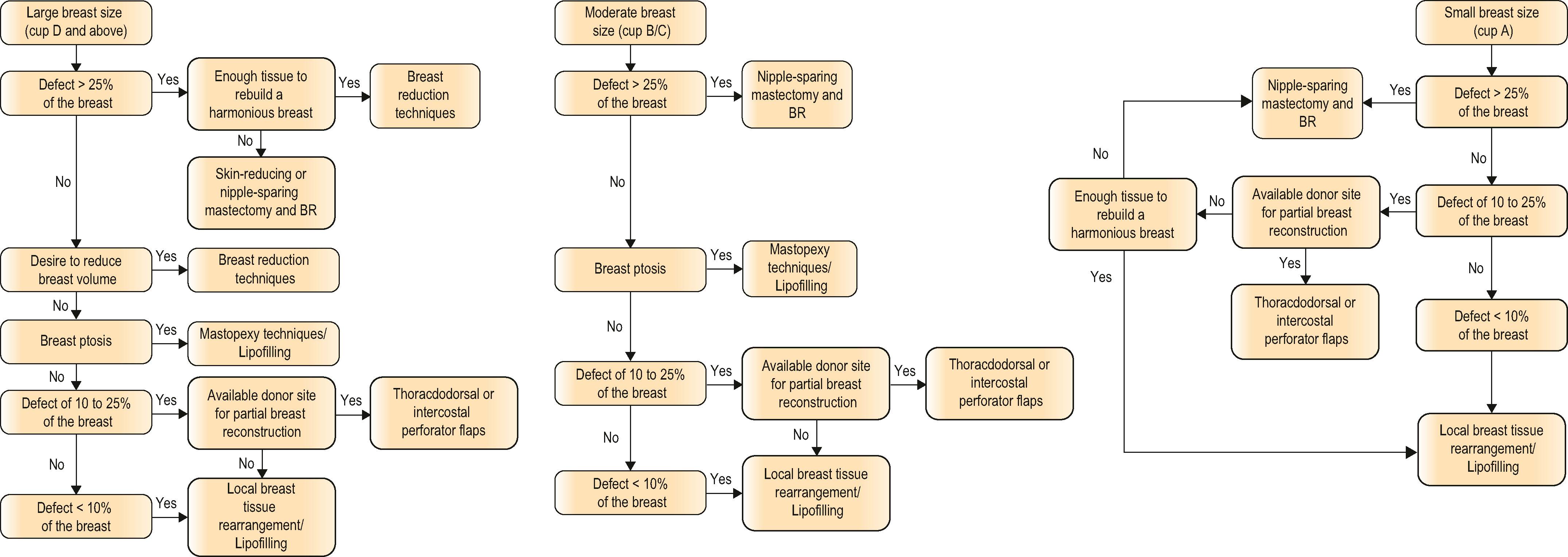
Several classification schemes have been developed to characterize breast deformity and suggest reconstructive options. The indications for each technique depend on four factors: breast size, degree of breast ptosis, defect size, and defect location. Defects of up to 10% can usually be repaired by local breast tissue rearrangement. Women with large breasts (D cup and above), or moderate breast size (B/C cup) with ptosis, are the best candidates for an oncoplastic approach, because a larger excision can be performed, giving a higher probability of obtaining adequate margins. In these cases, reduction mammoplasty and mastopexy are the most frequently used techniques to repair defects of up to 25% of the breast. In women with moderate breast size (B/C cup) without ptosis, or smaller breasts (A cup), repair defects between 10% and 25% of the breast can be challenging. Given that the breast volume and shape are usually adequate, tissue replacement techniques are the most frequently recommended procedures. Nevertheless, when planning to resect a larger tumor, affecting more than 25% of the breast, a nipple-sparing mastectomy and immediate reconstruction should be considered ( Algorithm 48.1 ).
Repair of the defect after breast-conserving surgery can be performed at the time of tumor resection (immediate repair), or weeks afterwards, when the final pathology margins are confirmed to be clear, but always before RT (staged-immediate repair). Alternatively, reconstruction of partial defects can be performed several months or years after breast-conserving surgery (delayed repair) ( Fig. 48.3 ). There are several advantages to operating on radiation-naive tissues. These include improved viability of any parenchymal rearrangement, greater pliability of local tissues and increased ease of pedicled flap reconstruction. Reconstruction of partial defects prior to RT is associated with a lower complication rate and fewer operations, and therefore, a better aesthetic outcome and high levels of patient satisfaction. Moreover, immediate reconstruction will reduce the psychological impact from any deformity consequent to breast-conserving surgery. In addition, whenever necessary, the correction of macromastia and breast ptosis will yield the benefit of aesthetic improvement and better adjuvant RT dose homogeneity. Since the reconstructive procedure seems not to influence the effectiveness of adjuvant RT on local control rates in breast cancer patients, repair of the defect should always be performed prior to RT. Surgical manipulation of an irradiated breast is associated with a greater number of operations, higher complication rates and less favorable aesthetic outcomes. Furthermore, the advent of intraoperative partial breast irradiation makes immediate repair the best approach. Delaying breast repair until after RT is no longer an advisable approach when planning breast-conserving therapy.

Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here