Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Metastases —prostate and breast most common. Heterogeneous; generally not diffuse.
Sickle cell disease —medullary sclerosis and bone infarcts. Growth arrest of long bones. H-shaped vertebrae.
Myelofibrosis —older patients. Diffuse medullary sclerosis, loss of corticomedullary differentiation. No heterogeneity.
Renal osteodystrophy —axial > appendicular. Rugger jersey spine.
Osteopetrosis —thickened cortices with reduced marrow space. Pathological transverse fractures.
Paget's disease —coarse trabeculae and bone expansion. Multiple bones rather than generalized.
Systemic mastocytosis —lytic, sclerotic or mixed. Usually diffuse affecting spine and epiphyses of long bones.
Fluorosis —diffuse osteosclerosis, particularly ribs and spine, with entheseal ossification.
Pyknodysostosis —narrow medullary cavities with multiple long bone fractures.
Hypoparathyroidism —diffuse sclerosis in 10%. Dense metaphyseal bands and skull vault thickening.
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) —young patients. Fusiform enlargement and sclerosis of long bones sparing the epiphyses.
Myeloma —rare osteosclerosing form. Associated with POEMS syndrome.
Bone island (enostosis) —ovoid with long axis parallel to long axis of bone and a feathered border.
Enchondroma —confluent punctate or nodular calcification, denser centrally than peripherally. Enchondromas in the large long bones are often more calcified than those in the fingers.
Metastasis —prostate, breast, mucinous adenocarcinoma of GI tract, carcinoid, lymphoma, TCC in adults. Medulloblastoma and neuroblastoma in children.
Callus —usually associated with a fusiform swelling in long bones.
Bone infarct —usually a central metadiaphyseal lucency with thin serpentine calcified margins.
Paget's disease —blastic phase causes sclerosis accompanied by bone expansion, and cortical and trabecular thickening.
Osteoma —arises from membranous bone: skull and paranasal sinuses. Ivory osteomas contain no trabeculae. Mature osteomas have visible marrow. If multiple consider Gardner syndrome.
Osteoid osteoma/osteoblastoma —sclerosis caused by eccentric periosteal thickening. Osteoid osteoma: radiolucent nidus <2 cm. Osteoblastoma: more common in the posterior elements of spine, larger nidus with thin shell.
Healed or healing bone lesion —treated metastasis, NOF, simple bone cyst, brown tumour, eosinophilic granuloma.
Primary bone sarcoma —aggressive features: poorly defined margins, aggressive periosteal reaction, Codman's triangles, bone destruction, soft tissue mass.
Fibrous dysplasia —usually lytic with ground glass areas but can calcify in later life.
Chronic osteomyelitis —usually associated with an area of lysis, chronic periosteal reaction and occasionally a sequestrum.
Chronic recurrent multifocal osteomyelitis (CRMO) —idiopathic inflammatory disorder. Most commonly affects clavicles and tibias in children. Often multifocal.
Lymphoma —primary bone lymphoma rare. More common as secondary involvement. Large extraosseous soft tissue mass with relative preservation of bone.
Cement and bone graft substitutes —history of surgery.
Metastases —prostate, breast, mucinous adenocarcinoma of GI tract, carcinoid, lymphoma, TCC in adults. Medulloblastoma and neuroblastoma in children.
Multiple healed bone lesions —lytic metastases following radiotherapy or chemotherapy. Eosinophilic granulomas and brown tumours following treatment.
Paget's disease —often polyostotic.
Multiple bone infarcts —consider an underlying disorder, e.g. sickle cell or Gaucher disease.
Multiple stress fractures —callus formation around fractures.
Lymphoma .
Osteopoikilosis —multiple symmetrically distributed bone islands in the metaphyses and epiphyses of long bones and the pelvis. Some ovoid, some round.
Multifocal osteosarcoma .
Multiple osteomas —Gardner syndrome.
Fibrous dysplasia —long lesions in long bones, often hemimelic (McCune-Albright syndrome). Usually lytic but can calcify.
CRMO and SAPHO .
Osteopathia striata (Voorhoeve disease) —linear striations along long axis of long bone.
Erdheim-Chester disease —bilateral symmetrical metadiaphyseal sclerosis in long bones, most commonly femora and tibias.
Multiple myeloma —sclerotic in 3%.
Tuberous sclerosis.
Intramedullary osteosclerosis —diaphyseal endosteal sclerosis typically involving the tibia or femur, usually bilateral and in women.
Healing fracture .
Metastasis —osteoblastic metastases from prostate.
Osteoid osteoma/osteoblastoma —solid or lamellated periosteal reaction.
Chronic osteomyelitis —look for sequestrum.
Osteosarcoma —classically sunray spiculation.
Ewing sarcoma —often onion-skin or lamellated periosteal reaction.
Chondrosarcoma —chondroid matrix with regions of enchondral ossification.
Lymphoma .
CRMO —clavicles and tibias in children and adolescents.
SAPHO syndrome —similar to CRMO but in adults. Although similar long bone changes may be seen, anterior chest wall and pelvic involvement predominate.
Infantile cortical hyperostosis (Caffey's disease) —infants <6 months of age. Multiple bones, especially mandible, ribs and clavicles.
Melorheostosis —sclerotomal distribution. Cortical and medullary sclerosis likened to dripping candle wax.
Tertiary syphilis —usually bilateral periostitis involving skull, clavicles, ribs and tibias. Mixed sclerotic and lytic ‘gummatous’ lesions can also be seen.
Osteoid osteoma/osteoblastoma —lucent nidus.
Brodie's abscess .
Medullary bone infarct —irregular serpentine outline.
Stress fracture —lucent fracture line may be visible.
Looser's zone of osteomalacia .
Liposclerosing myxofibrous tumour —characteristic location in the intertrochanteric region of the femur.
Tuberculosis .
Syphilis.
Yaws.
Paget's disease .
Osteoporosis .
Osteomalacia .
Haemoglobinopathies .
Haemangioma .
Gaucher disease.
Nearly all malignant tumours can metastasize to bone, but 80% are from prostate, breast, lung or kidney. Mainly involves the axial and proximal appendicular skeleton (red marrow)—distal appendicular bone metastases are rare and usually from lung or, less commonly, breast. Most bone metastases are lytic; sclerotic or mixed metastases have a more limited differential, though treated lytic metastases can become sclerotic. The lists below cover the more common sources.
Lung .
Breast —usually lytic but can be sclerotic or mixed.
Myeloma .
Nonmucinous adenocarcinomas of the GI tract .
Most other primary sources .
Renal cell carcinoma .
Thyroid .
Hepatocellular carcinoma.
Melanoma.
Phaeochromocytoma.
Prostate .
Breast — particularly post treatment.
Carcinoid.
Mucinous adenocarcinomas of the GI tract.
Transitional cell carcinoma.
Small cell lung cancer.
Lymphoma —particularly Hodgkin lymphoma; rare.
Breast .
Lung .
Lymphoma .
Cervix.
Testis.
Transitional cell carcinoma.
Melanoma.
Neuroblastoma —in children.
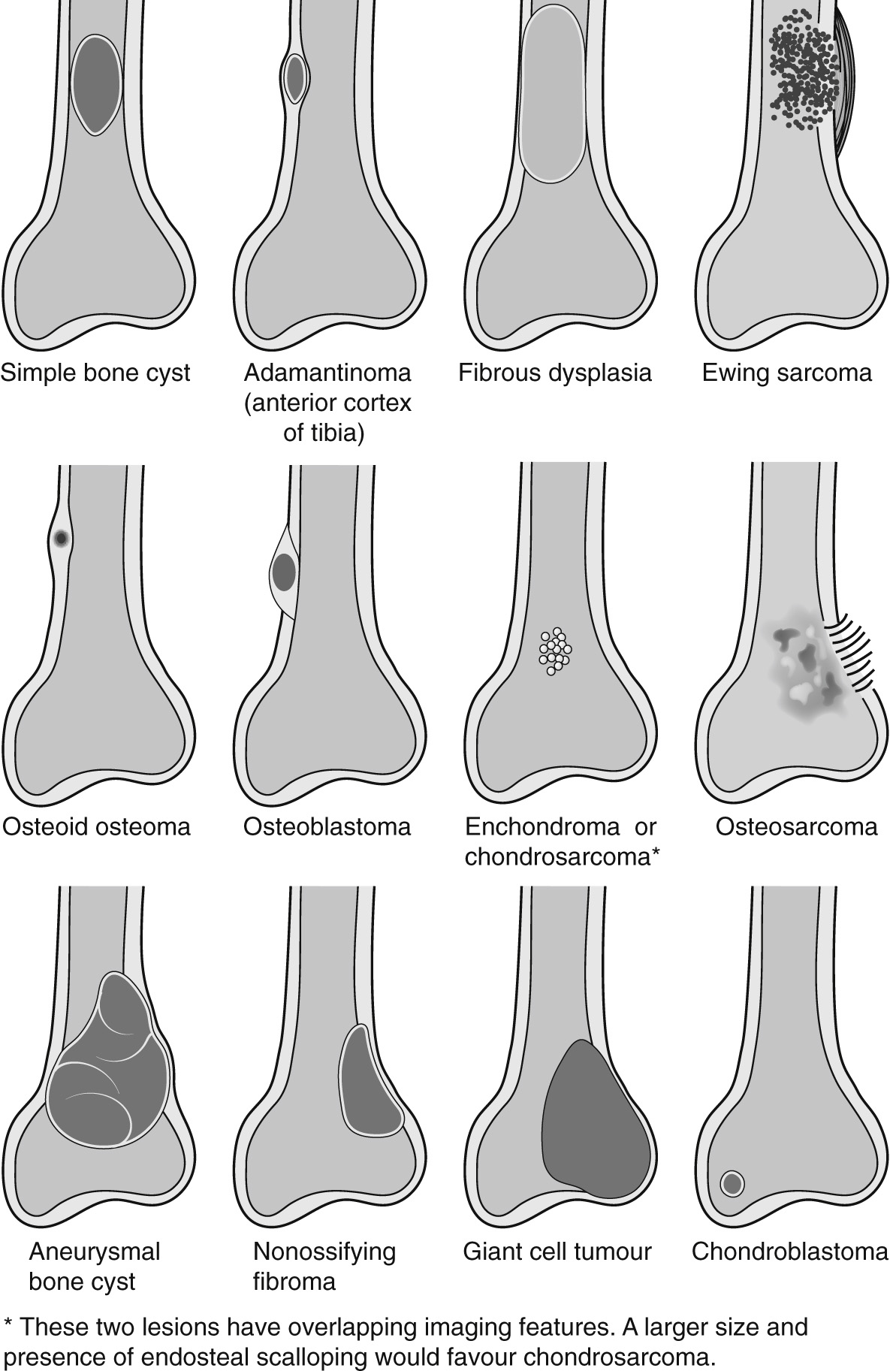
| Peak age (years) | Location | Centrality a | Density | Margin | Expansile a | Periosteal Reaction b | Notes | |
|---|---|---|---|---|---|---|---|---|
| Generally well-defined predominantly lytic lesions | ||||||||
| Simple bone cyst | 5–20 | Met±Dia | Central | Lucent | Well+Scl | −/+ | − | Unilocular. ‘Fallen fragment’ if fractured |
| Aneurysmal bone cyst | 5–30 | Met | Eccentric | Lucent | Well+Scl | ++ | − | Expansile, bubbly . May occur 2° to another lesion |
| Giant cell tumour | 20 – 50 | Met+Epi | Eccentric | Lucent | Well/Poor | + | − | Nonsclerotic margin, often abuts articular surface |
| NOF/FCD * | 5–25 | Met | Cortical | Lucent | Well+Scl | −/+ | − | NOF >3 cm; FCD <3 cm. Sclerose after healing |
| Benign fibrous histiocytoma | 25 – 40 | Met/Dia | Eccentric | Lucent | Well±Scl | −/+ | − | Rare; similar to NOF but in older patients + any location |
| Chondromyxoid fibroma | 10–30 | Met | Eccentric | Lucent | Well±Scl | + | − | Rare; can mimic NOF, ABC and BFH |
| Osteoid osteoma | 10–30 | Dia /Met | Cortical | Lucent±Ost | Scl | - | Solid | Lucent nidus <2 cm + surrounding sclerosis |
| Osteoblastoma | 10–30 | Dia/Met | Eccentric | Lucent±Ost | Well±Scl | + | Solid | Lucent nidus >2 cm ; spine > flat bones>long bones>talus |
| Chondroblastoma | 5–20 | Epi | Eccentric | Lucent±Chon | Well+Scl | − | −/Solid | Classically epiphyseal ; also in apophyses, patella, tarsals |
| Intraosseous lipoma | >20 | Met | Any | Lucent±Scl | Well±Scl | −/+ | − | Lucent ± central sclerosis . Calcaneus >prox femur>other |
| Fibrous dysplasia * | >3 | Dia | Central | Ground glass | Well±Scl | + | − | Variable density. Commonest in long bones, ribs, skull |
| LSMFT | >20 | Met | Central | Lucent ±Scl | Well+Scl | −/+ | − | Intertrochanteric region of femur |
| Adamantinoma | 10–35 | Dia | Cortical | Lucent ±Scl | Well+Scl | + | − | Anterior cortex of tibial diaphysis |
| Osteofibrous dysplasia | <10 | Dia | Cortical | Lucent±Scl | Well±Scl | + | − | Similar to adamantinoma but in younger age group |
| Desmoplastic fibroma | 10–50 | Met/Dia | Central | Lucent | Well | + | − | Rare. Lytic + pseudotrabeculations |
| Haemophilic pseudotumour | >10 | Any | Any | Lucent | Well±Scl | ++ | − | Male ± signs of haemophilia ± pseudotrabeculations |
| Brown tumour | >40 | Any | Any | Lucent | Well | + | − | Look for other features of hyperparathyroidism |
| Generally well-defined sclerotic/mixed lesions | ||||||||
| Bone island | >20 | Any | Any | Scl | Well | − | − | Round/oval ± spicules, uniformly dense, <2 cm |
| Bone infarct c | Any | Any | Central | Scl +Lucent | Well+Scl | - | − | Serpiginous sclerosis , can mimic enchondroma |
| Enchondroma * | >10 | Met/Dia | Central | Lucent/Chon | Well | −/+ | − | Lytic in phalanges, chondroid calc in larger bones |
| Chondrosarcoma d | >30 | Met | Central | Lucent/Chon | Poor/Well | −/+ | − | Can mimic enchondroma, chondroblastoma or GCT |
| Haemangioma * , e | >10 | Met | Any | Lucent±Scl | Well | −/+ | −/Spic | Spine > skull > other. Appearance depends on site |
| Paget's disease | >40 | All | All | Lucent/Scl | Well | − | − | Appearance depends on stage and location; see Part 2 |
| Aggressive lesions in children and adolescents | ||||||||
| Osteomyelitis | Any | Met/Epi | Any | Lucent | Poor | − | Lam | If chronic: sclerosis ± sequestrum ± cloaca |
| Brodie's abscess | 0–20 | Met/Epi | Any | Lucent | Scl | − | Solid | Discrete lucency + surrounding sclerosis |
| Eosinophilic granuloma | 0–30 | Any | Any | Lucent | Poor/Well | − | Lam | Variable site/appearance, usually aggressive |
| Ewing sarcoma | 5–20 | Dia | Central | Mixed | Poor | − | Lam | Often subtle, ± noncalcified soft tissue mass |
| Osteosarcoma f | 10–25 | Met | Any | Ost | Poor | − | Spic | ± Characteristic osteoid matrix in soft tissue mass |
| Aggressive lesions in adults | ||||||||
| Metastasis | >40 | Any | Any | Lucent/Scl | Poor/Well | −/+ | −/Spic if sclerotic | Usually multiple, variable appearance; see Section 1.7 |
| Plasmacytoma | >40 | Any | Central | Lucent | Well | ++ | − | Axial and proximal appendicular skeleton |
| Bone lymphoma | >30 | Any | Central | Mixed | Poor | − | Lam | Large soft tissue mass + only subtle bone changes . 2°>1° |
| Chordoma | >30 | N/A | Central | Lucent+ Scl | Well±Scl | ++ | − | Lytic + foci of calcification. Sacrum > clivus > vertebrae |
| Fibrosarcoma and UPS | >20 | Met/Dia | Any | Lucent | Poor | − | Any | Nonspecific. Can arise from Paget's, infarct and others |
| HP/HE/angiosarcoma | >20 | Any | Any | Lucent | Poor | + | − | Rare. A regional cluster of lytic lesions is suggestive |
* These lesions, when in their polyostotic form, often occur in atypical locations and have atypical appearances; e.g. Jaffe-Campanacci syndrome (NOFs), McCune-Albright syndrome (fibrous dysplasias), Ollier disease and Maffucci syndrome (enchondromas), cystic angiomatosis (haemangiomas).
a Note that eccentric and nonexpansile lesions may appear central and expansile if large or within a small/thin bone.
b Note that any lesion may show a periosteal reaction if fractured.
c Note that acute bone infarcts are usually occult on plain film. If seen in children, suspect underlying sickle cell or Gaucher disease. Termed avascular necrosis when located in the epiphysis. Bone infarcts can transform into various sarcomas.
d Low-grade chondrosarcomas can occur in young adults and can look nonaggressive or mimic enchondroma—features favouring chondrosarcoma include size >5 cm, deep endosteal scalloping or cortical breach, atypical location (e.g. pelvis, axial skeleton, epiphysis) and history of pain. The clear cell variant of chondrosarcoma arises in epiphyses and can mimic chondroblastoma (though usually in an older age group). Chondrosarcomas can also arise from an existing enchondroma or osteochondroma.
e Vertebral haemangiomas are common and show coarse vertical trabeculae. In flat bones haemangiomas are often expansile with a sunburst periosteal reaction. In long bones the trabecular coarsening often creates a honeycomb appearance.
f Osteosarcoma has a second peak in old age due to malignant degeneration of other lesions, e.g. Paget's disease, bone infarct, fibrous dysplasia. Also beware the telangiectatic variant (mimics ABC).
Nonossifying fibroma —young patients, eccentric metaphyseal location. Consider benign fibrous histiocytoma if patient >25 years or atypical location.
Bone cysts — both SBCs and ABCs usually have a thin sclerotic margin. ABCs are more eccentric and expansile.
Fibrous dysplasia — variable appearance, typically diaphyseal.
Chondroblastoma —epiphyseal location, young patients. If patient >20 years, consider clear cell chondrosarcoma.
Brodie's abscess —typically young patients, most common in metaphysis. Discrete lucency with surrounding ill-defined sclerosis.
Healing metastases or primary malignant bone lesions — sclerotic rim indicates a good response to treatment.
Osteoblastoma — large lucent nidus with a sclerotic margin. Most common in spine.
Intraosseous lipoma — typically in calcaneus or intertrochanteric region of femur. Thin sclerotic margin. Focus of central calcification is pathognomonic but not always present.
Liposclerosing myxofibrous tumour — characteristic location: intertrochanteric region of femur. Usually a thick sclerotic margin.
Adamantinoma/osteofibrous dysplasia (OFD) — characteristic location: anterior cortex of tibial diaphysis. Both can look identical but OFD occurs in a younger age group (<10 years).
Chondromyxoid fibroma— rare; can mimic NOF, BFH and ABC.
Haemophilic pseudotumour— usually very expansile + other signs of haemophilia.
Metastasis — usually older patients, in axial or proximal appendicular skeleton.
Myeloma/plasmacytoma —older patients, usually in axial or proximal appendicular skeleton. Typically ‘punched-out’ appearance, may be expansile.
Low-grade chondral lesions —e.g. enchondroma, low-grade chondrosarcoma. Both can be lytic without chondroid matrix.
Giant cell tumour —typically has a well-defined nonsclerotic margin. Adults 20–50 years.
Simple/aneurysmal bone cyst —both may have no perceptible sclerotic margin.
Eosinophilic granuloma —may appear well-defined.
Brown tumour —often expansile. Look for other signs of hyperparathyroidism.
Lytic phase of Paget's disease —well-defined flame-shaped advancing edge without sclerosis.
Desmoplastic fibroma —rare. Often contains pseudotrabeculations.
Metastasis —usually ill-defined.
Myeloma —usually discrete but may appear ill-defined.
Osteomyelitis —ill-defined and lytic in the acute phase.
Bone lymphoma — typically ill-defined subtle bone destruction with a large soft tissue mass. Can occur at any age but more common in older patients.
Primary bone sarcomas —e.g. Ewing sarcoma, osteosarcoma, chondrosarcoma, fibrosarcoma, undifferentiated pleomorphic sarcoma, angiosarcoma. Internal matrix may be absent.
Eosinophilic granuloma —patients <30 years. Can occur anywhere, often has an aggressive appearance indistinguishable from infection or malignancy.
Giant cell tumour —can appear ill-defined. Adults 20–50 years.
Plasmacytoma —older patients, usually in axial or proximal appendicular skeleton.
Metastases —RCC, thyroid, HCC, phaeochromocytoma, melanoma. Usually in axial or proximal appendicular skeleton.
Aneurysmal bone cyst —in children and young adults. Usually has a thin sclerotic margin.
Giant cell tumour —usually older patients than ABC. Often abuts articular surface, no sclerotic margin.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here