Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Male and female aesthetic genital surgery can greatly enhance confidence if a real or perceived deformity exists.
Many new genital surgeries have been developed.
In the male, penile enlargement surgery can result in severe deformities, which can often be reconstructed.
Hidden penis, penoscrotal web, and scrotum reduction surgeries are very successful with a low complication rate.
Labia minora and clitoral hood reduction performed by the “extended central wedge” excision gives a natural appearance with very high patient satisfaction.
Mons pubic lifting and labia majora reduction, with or without fat excision, increase self-esteem.
As with all aesthetic surgeries, genital surgery requires the same meticulous attention to detail.
 Access video lecture content for this chapter online at Elsevier eBooks+
Access video lecture content for this chapter online at Elsevier eBooks+
Identity and self-esteem are intimately related to a person's image of his or her genitalia. Self-esteem can be impaired if a person feels inadequate compared with a perceived ideal. A normal man may consider his penis to be too small or a woman may judge her genital appearance as unsightly. These feelings develop from self-comparisons with pornographic photos or videos, media attention, or comments from a sexual partner or friend.
Patient awareness has led to significant demand for aesthetic genital surgery. Recently, new techniques to enhance the appearance of male and female genitalia have been developed, based partially on improved reconstructive pediatric and adult surgical procedures. Considerable aesthetic improvement in the genital appearance is now possible. The surgery is challenging and requires strict attention to detail and meticulous technique (  ).
).
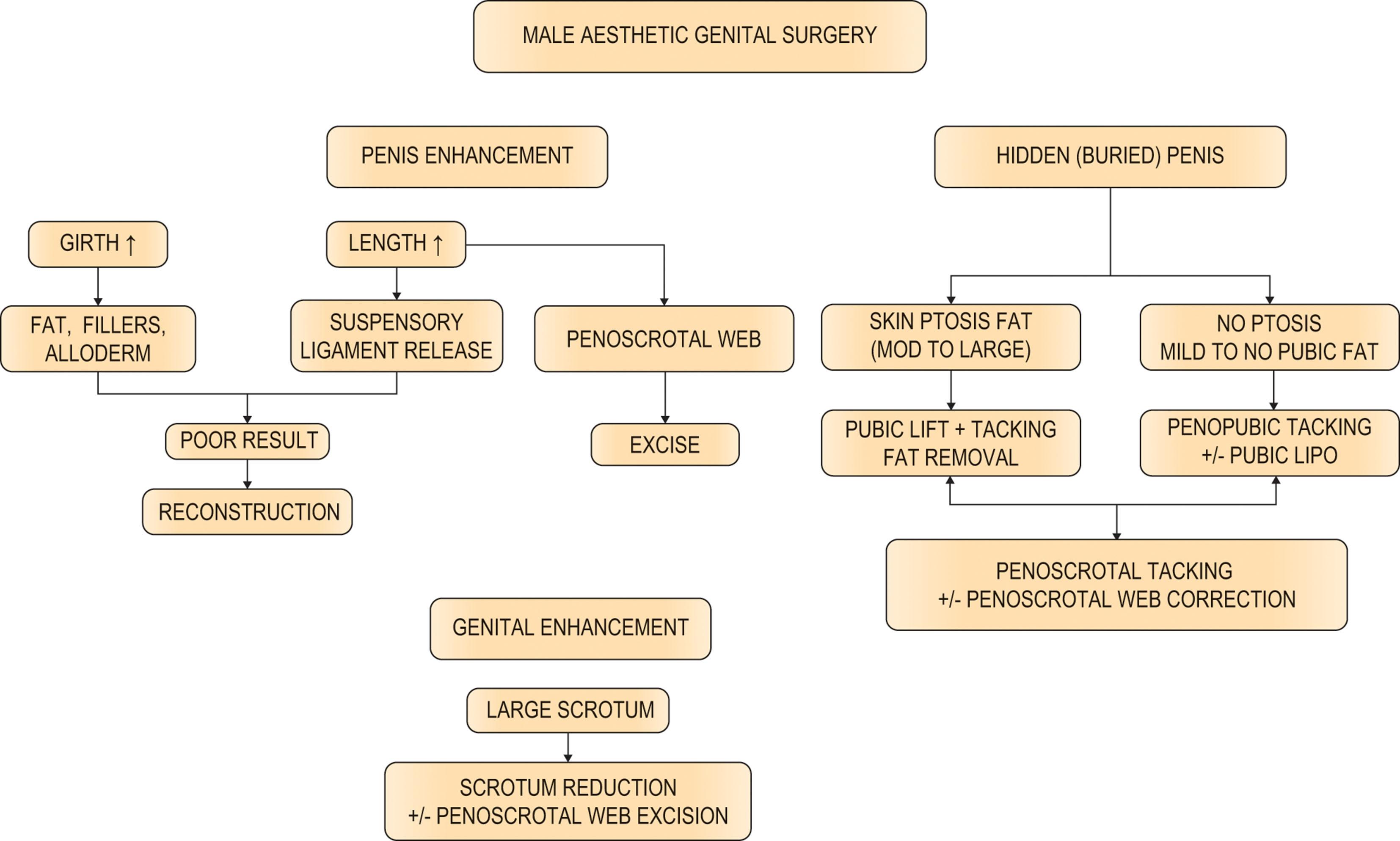
Several procedures are now available to enhance or improve the aesthetic appearance of the penis or scrotum, as summarized in Algorithm 40.1 . Penile lengthening is performed by releasing the suspensory ligament of the penis followed by the use of penile weights or stretching devices. Penile girth is increased by either injecting fat or foreign substances or by inserting dermal fat grafts or allografts such as acellular dermal matrix into the dartos fascia. Penoscrotal webbing may be corrected with one or several Z-plasties, usually combined with excision of the web skin. An enlarged, low-hanging scrotum can be reduced and lifted. The hidden or buried penis is corrected with suprapubic fat removal, possible upper pubic skin resection, and stabilization of pubic and penoscrotal skin.
Men are very resistant to psychiatric evaluation prior to penile enlargement surgery. Many of the men presenting for penile enlargement have significant generalized self-esteem issues, so refusal to perform the surgery may be justified. The psychological motivations of a man with a hidden penis, penoscrotal webbing, scrotal enlargement, or true congenital deformities are different from those of a man with a normal-sized penis who desires only enlargement, so his care is usually more rewarding for both the patient and the surgeon.
Schonfeld and Beebe determined that the length of the fully stretched flaccid penis correlated closely with the erect penis. The dorsal length from the junction of the penopubic skin to the tip of the glans in the fully stretched flaccid penis correlated closely to the erect penis. Erect girth or circumference correlated with girth measurements of the flaccid penis according to a more complicated ratio.
Da Ros et al . performed artificial erections on 150 men of European origin, measuring penis length from the center of the pubic bone to the tip of the glans and penis circumference at the corona and base. Average penis length was 5.7 inches (14.5 cm); 18 were shorter than 4.7 inches (12 cm) and 18 longer than 6.3 inches (16 cm). Circumference at the base of the penis ranged from 3.5 to 5.9 inches (8.9–15 cm) (average 4.7 inches [11.9 cm]) and at the coronal groove from 3.2 to 5.5 inches (8.1–14 cm) (average 4.4 inches [11.2 cm]).
Wessells et al . compared the relationship between penile length in the flaccid stretched and the erect states and also concluded that there was a positive relationship. The average flaccid stretched penile length was 11 cm, while the average erect penile length was 12.5 cm. The correlation between stretched length and erect length was r 2 = 0.769. Average flaccid circumference was 10 cm with an average erect circumference of 12.5 cm, and, therefore, correlation was not favorable for circumference. They also state that a thick pubic fat pad decreases visible flaccid penile length but not functional penile length during intercourse.
The patient is evaluated both standing, sitting, and supine to determine variations that change with gravity. While standing, the penis is checked for concealment owing to descent of the pubic fat pad and escutcheon from gravity, since supine positioning often eliminates this abnormality. If the penis disappears when sitting or bending down, this is a sign of a buried penis. A protuberant abdomen with excess skin and fat may overhang the penis and functionally interfere with sexual intercourse, so the patient may need an abdominoplasty or panniculectomy in addition to a suprapubic lipectomy and skin excision. The amount of suprapubic fat between the pubic symphysis and the skin should be evaluated to determine potential length improvement from suprapubic lipectomy or liposuction. Penis position must be checked to see if it is partially encircled by the scrotum. The underside of the penis should be examined for penoscrotal webbing that causes an aesthetically or functionally shorter penis. Supine measurements are taken from the pubic bone and from the skin over the pubis to the tip of the glans on full stretch while the penis is at 90° to the abdomen. Circumference is measured at the base and corona with the penis on full stretch. The penis should be palpated for Peyronie's plaques, which are firm scars on the tunica albuginea.
It is important to question and evaluate function prior to penile surgery. Urinary and orgasmic function should be normal and neither is affected by these procedures.
The patient is asked if he has any erectile difficulties or penile curvature. Most men have some minor curvatures, but these are not bothersome and are not an issue. However, if girth surgery is considered, any known or suspected curvature should be documented. The patient is asked to present photographs showing his erect penis from various angles. If the patient is unwilling to present photographs, an erection can be obtained, and then photographed, by patient self-stimulation or by intracavernosal injection of prostaglandin E1. This pharmacologic agent is injected with a 30-gauge needle transversely into the cavernosal bodies at the base of the penis. The injected dosage usually is 10 µg in the normal male. The patient should be cautioned about the possibility of priapism and the necessity for mandatory reversal of the erection if it persists longer than 4 h. The erection can be immediately reversed with a low-dose intracavernosal injection of phenylephrine, which is routinely performed to reverse a pharmacologic erection at the end of surgery.
Once the diagnosis is made, the possible procedures are discussed with the patient, as well as risks and benefits. Penoscrotal webbing and extensive suprapubic fat and pubic descent may not be presenting complaints, but the physician must describe these abnormalities and possible corrective surgery. Each individual is evaluated to determine the best method to achieve his goals, since several procedures are available depending on the patient's anatomy. He must have a realistic understanding of the design and limitations of the surgery in order to prevent misconceptions and dissatisfaction. Exaggerated promises lead to patient disappointment, depression, and hostility; therefore, honesty, clear communication, and compassion are mandatory for both patient and physician. Because not all malpractice carriers will cover physicians for penile enlargement procedures, verification of coverage is recommended.
The suspensory ligament of the penis is a thick, triangular band extending from the linea alba and the upper portion of the symphysis pubis and arcuate ligament to the dorsal midline of the penis. It derives from the outer investing fascia of the abdomen and divides into a sling at the junction of the fixed and mobile portions of the penis. In addition, thickened bands of Scarpa's fascia, called the fundiform ligaments, firmly attach to the rectus fascia above the pubic symphysis and extend onto the dorsal and lateral penis, possibly restricting penile excursion.
The skin of the penis is thin, hairless (more distal), and has loose connections with the deeper structures of the penis. No adipose tissue is present under the skin. The superficial or subcutaneous fascia of the penis (dartos fascia) is continuous with the Scarpa's and Camper's fascias of the lower abdomen and extends to the corona of the penis. The dartos fascia contains scattered smooth muscle cells. Branches of the superficial external pudendal vessels provide the blood supply to the dartos fascia and skin. The internal pudendal system, which includes the deep dorsal arteries and veins and the cavernosal and urethral vessels, usually communicates with the external pudendal system only at the glans and corona. Because the dartos fascia is highly vascular, it provides an excellent tissue bed for grafts. Buck's fascia invests the shaft of the penis deep to the dartos fascia. The dorsal nerves of the penis supply erogenous sensation to the glans penis. The deep dorsal vessels and the dorsal nerve travel in the pudendal canal along the ischial ramus and then pass ventrally along the margin of the inferior ramus of the pubis in the deep perineal pouch. The neurovascular bundles pierce the perineal membrane ½ inch from the symphysis pubis and continue within Buck's fascia of the penis. Each of the two deep dorsal arteries lie between the deep dorsal vein in the midline and the dorsal nerves of the penis laterally.
Penile lengthening is achieved by releasing the suspensory ligament of the penis and the postoperative use of penile weights or stretching devices ( Fig. 40.1A ). The ligament is released only one fingerbreadth by cutting directly on the periosteum throughout the length of the midline pubic symphysis. The release is usually performed through a 3–4 cm lower transverse incision just above the penopubic junction, but many surgeons advance infrapubic skin onto the penis using a V–Y advancement flap ( Fig. 40.1B,C ). This V–Y flap theoretically increases penile length or gives the penis the appearance of increased flaccid length, which may occur if the patient has a shortage of penile skin. Penile length gain is disputed in most cases, and the V–Y flap can actually cause the penis to appear either longer or shorter in the flaccid state. The V–Y flap is based distally at the penopubic junction varying from a small (2–3 cm) to a large base. The larger flap encompasses the entire dorsal base of the penis and part of the scrotum, which causes interruption of a significant portion of the proximal penile dartos fascia and skin. The blood supply and lymphatic drainage of the penis is thus partially interrupted, which can cause healing complications such as flap tip loss, poor wound healing with wound dehiscence, and postoperative swelling. Healing problems predispose to hypertrophic or wide scars, which create hairless pubic scars and depressions ( Figs. 40.2A & 40.3A ). The large V–Y flap also advances thick, hair-bearing tissue onto the penis, which frequently creates an unnatural hump at the penile base and the appearance of a low-hanging penis. The penis can appear surrounded by the scrotum (scrotalization) with an overhanging large pubic fat pad, which makes the penis look shorter and hidden. A V–Y flap can also create “dog-ears” at the distal scrotal flap incision. Smaller V–Y advancement flaps cause less frequent problems, but wound and aesthetic complications also occur.
 The suspensory ligament is released. (B) A large V–Y advancement flap is designed. (C) The flap is advanced, resulting in hair on the proximal penile shaft, bilateral dog-ears, and a lower-hanging penis.")
 The scar is marked for excision. The marking at the base of the V–Y flap on the left is the estimated location for the reapproximation of the flap to the pubic hairline. (B) Complete reversal of the V–Y flap resulting in a semicircular incision line. Hair on the V–Y flap is aligned with the pubic hair.")
 The deformity shows a low-lying penis, hair on the proximal shaft, bilateral dog-ears at the penoscrotal junction, a short-appearing penis, wide pubic scars, and fat in the shaft. (B) Reconstruction after partial reversal of the V–Y advancement flap, correction of the V–Y dog-ears, scar revisions, and selective removal of fat. Complete reversal of the V–Y flap was not possible due to previous partial loss of a portion of the V–Y flap.")
It is difficult to interpret the results of penile lengthening, because no standardized measurement technique exists, and no mainstream studies have been published.
Suspensory ligament release alone may rarely increase flaccid penile length 1–2 cm, but often no gain is achieved. Real flaccid and erect length gain may be obtained by using penile weights or penile stretching devices. Patients can use these devices without undergoing ligament release, but the ligament release frees more of the penis to be expanded, thereby possibly increasing the amount of eventual length gain. A patient should not undergo release of the suspensory ligament unless he is willing to use the stretching devices. Approximately 1 week after surgery, the patient suspends the weights or devices from the end of the penis several times daily over a period of months to years, stretching the corporal bodies. The amount of weight required as well as the duration and frequency of use are still evolving. Other devices are available to produce constant penile stretching and traction.
The amount of length gain achieved is controversial, and most patients probably do not achieve any significant increase even with stretching devices. Actual length gains of several inches are rare, but may occur if a suprapubic lipectomy is also performed on thick subcutaneous tissue. However, anecdotal flaccid as well as erect increases of several inches have been reported by some compulsive weight-users. In fact, a ½-inch to 1-inch gain is considered very successful, albeit very uncommon.
An occasional patient may complain of penile shortening after release of the suspensory ligament. Since there is a dead space between the pubic symphysis and the corpora, it is possible for the corpora to reattach in a shortened position. This dead space can be filled by a proximal- or distal-based fat flap transposed from the medial spermatic cord ( Fig. 40.4 ). However, most doctors tell the patients to stretch the penis after the release without filling the space.

Penile instability is very rare after suspensory ligament release and usually results from an overly aggressive release of the corporal bodies from the ischiopubic rami. If the release is limited to one fingerbreadth on the midline of the pubic symphysis, this will not occur. Dorsal nerve or vessel injuries are prevented by staying directly on the pubic periosteum of the midline of the symphysis with the penis on full stretch and by not releasing the corpora laterally. A mild decrease in the elevation of the erection can occur with release but is not problematic.
Techniques to increase penile girth are in a constant state of evolvement and are associated with the largest incidence of complications. The difficulty of achieving girth enhancement is the necessity to create a symmetrical, relatively cylindrical phallus. Any graft that may resorb can cause visual or functional deformities. Thus, many techniques have been used with varying success.
Simultaneous lengthening and girth enhancement procedures are not performed by some physicians because weight use needs to be delayed several weeks owing to penile swelling and discomfort, which risks premature ligament reattachment. Moreover, the complication rate increases if both operations are performed simultaneously, resulting in wound problems and decreased graft survival. A girth procedure is sometimes performed once length is achieved.
Autologous fat injections into the dartos fascia are still used by some physicians to increase penile thickness. The fat is moveable and gives a somewhat spongy texture to the penis. Less than 50% of injected fat normally survives in other parts of the body. Ideally, small amounts of fat (10–20 cc) are injected in multiple tunnels. Small amounts of total injected fat produce only minimal girth gain but do not have much risk of complications. Complications include asymmetry of the sides of the penis, nodules with bulging and concavities, and loss of penile rigidity due to an overabundance of fat (see Figs. 40.3 & 40.5A ).
 Patient with large volume of injected penile fat that is causing obvious convexities. (B) Circumcision incision reveals diffuse fat deposits. (C) Residual fat after contouring. (D) Penis appearance after closure. It is very difficult to achieve ideal symmetrical contouring.")
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here