Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Extensor tendon injuries are relatively common.
The mechanism of finger extension is more complicated than that of flexion. It is achieved through the synergistic action of both extrinsic and intrinsic muscles with contribution from several passive ligamentous structures.
Extensor tendons over the fingers are thinner, flatter, and lie closer to bony structures than flexor tendons ( Fig. 82.1 ).

Surgical treatment is considered for most open injuries and for closed injuries proximal to the proximal interphalangeal (PIP) joint.
Specific considerations apply to each zone of injury.
Extensor tendon repair should not be attempted in the setting of active or suspected infection.
Severe joint contractures and patient inability to comply with the postoperative rehabilitation protocol are also relative contraindications to extensor tendon repair.
The Elson test ( Fig. 82.2A ) may detect a closed central slip injury. The patient should flex the PIP joint 90 degrees over the edge of an examination table and try to actively extend the PIP joint against resistance by the examiner or against a flexed finger of the contralateral hand (see Fig. 82.2B-E ). As the patient attempts PIP joint extension (but kept at 90 degrees by resistance), tension across the distal interphalangeal (DIP) joint is assessed. If the central slip is ruptured, the DIP joint will be tight or will hyperextend because of increased tension across the lateral bands and terminal tendons with attempted digit extension. When the central slip is intact, it acts as a checkrein to prevent proximal lateral band motion and the DIP joint remains relaxed during resisted extension of the PIP joint.
 Elson test. The red arrow indicates the examiner resisting proximal interphalangeal joint extension. (B–E) Illustration of examiner performing Elson test.")
A plain radiograph is required to exclude a fracture, foreign body, or other bone and joint abnormalities.
A commonly used classification of extensor tendon injury level was described by Kleinert and Verdan ( Fig. 82.3 ).

Extensor tendons from the level of the DIP joint to the wrist joint are categorized into zones, which go from I to VII.
Each joint corresponds with the odd numbered zones: zone I overlies the DIP joint, zone III overlies the PIP joint, and so on. (TI indicates the thumb interphalangeal [IP] joint, TIII the thumb metacarpophalangeal [MCP] joint, and TV the level of the extensor retinaculum).
The extensor indicis proprius (EIP) and the extensor digiti minimi (EDM) tendons permit independent extension of the index and small fingers. For that reason, isolated injuries of the EIP or EDM tendons do not always need to be repaired ( Fig. 82.4 ).

The juncturae tendinae are stout bands that connect the ring finger extensor tendon to the middle and small finger tendons over the hand. There is also a less substantial band between the index and middle finger. With proximal extensor tendon injuries, the patient may still be able to extend the finger to a degree through the adjacent junctura.
The surgeon must be aware of the numerous patterns of aberrant extensor anatomy, including the possible presence of extensor carpi radialis intermedius, extensor medii proprius, extensor digitorum brevis manus, and others. These accessory tendons may be sources of graft if needed.
Appropriate anesthesia is required for wound exploration or tendon manipulation. Use local or digital blocks for injuries in zones I to IV and field or regional nerve blocks for injuries in zones V to VII.
A wide-awake approach is recommended in select patients with extensor tendon injuries to evaluate the strength of the tendon repairs and immediate motion (see Chapter 77 ).
In general, the suture method of extensor tendon repair depends on the tendon thickness at the level of injury. Extensor tendons become thin and flat distally.
Commonly used core suture techniques, based on surgeon preference, include horizontal mattress, figure of eight, modified Bunnell, and modified Kessler techniques ( Fig. 82.5A–D ).

Many studies have been undertaken to establish the best suture techniques for each zone, and techniques with the greatest load strength include a running interlocked horizontal mattress ( Fig. 82.6A–B ), the modified Bunnell, modified Kessler, and modified Becker techniques. The extensor tendons are thin and flat, however, and so it can be difficult to apply complicated suture techniques.
 Running interlocked horizontal mattress.")
We prefer a four- to six-strand horizontal mattress repair using a 3-0 or 4-0 braided suture for most extensor tendon lacerations.
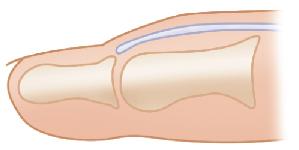
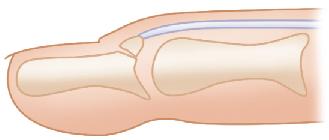
According to Doyle’s classification of mallet finger injuries ( Table 82.1 ), type I (closed) injury ( Fig. 82.7 ) is the most common and is managed nonoperatively with continuous splinting of the DIP joint for 6 to 8 weeks. A mallet deformity can be improved by splinting up to 6 months from the injury, but this treatment may be less effective with chronic deformities.

If the type I mallet deformity remains after 8 weeks of splinting, additional splinting can be attempted or surgical treatment (such as simple Kirschner wire [K-wire] fixation of the DIP joint) can be applied.
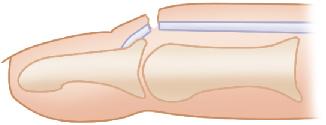
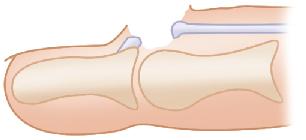
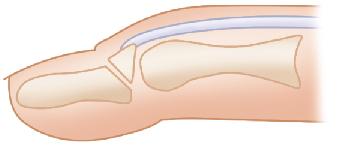
Type II, III (open injury), and unstable type IV (mallet fracture) injuries generally require surgical treatment. Type IVB may be treated conservatively if there is no DIP joint subluxation or instability.
Patients who are unable to comply with uninterrupted splinting of a mallet deformity may be treated with K-wire fixation of the DIP joint.
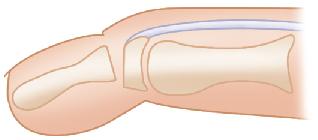
Fix the DIP joint in a slightly hyperextended position using one or two 0.045-inch (1.14-mm) K-wires in a retrograde fashion ( Fig. 82.10 ).
.")
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here