Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Abdominolipoplasty is a system of classification and treatment for abdominal contour surgery based on the treatable soft-tissue layers of skin, fat, and muscle of the abdominal wall.
Lipoabdominoplasty is a modification of traditional abdominoplasty that incorporates liposuction of the underlying flap and potentially other areas. The safety of lipoabdominoplasty is based on the manner in which the flap is undermined (inverted “V” style), extent of liposuction, and degree of liposuction, as well as the tension on wound closure.
Complications in abdominoplasty have been reported as local versus systemic, and early or late. Numerous databases for complications exist, and depending upon what they capture, the findings may vary.
Venous thromboembolism occurs more often in abdominoplasty than in other aesthetic procedures. Consequently, screening for high-risk situations, risk modifications, perioperative (pre- and intraoperative) prophylaxis, and postoperative surveillance should be instituted and are essential in these patients.
Depending upon a patient’s goals and anatomy, there are other abdominal contour procedures available. These less-invasive procedures, known as “downstaging,” can be considered, but do not yield the same result as a full abdominoplasty.
Secondary full abdominoplasty means the first operation was different (i.e., liposuction or limited abdominoplasty), or due to age, pregnancies, or unsatisfactory results after a primary abdominoplasty, then the second operation. A revision of a procedure refers to a re-operation by the original surgeon for a complication, unsatisfactory result, or the need for further improvement.

 Access video and video lecture content for this chapter online at Elsevier eBooks+
Access video and video lecture content for this chapter online at Elsevier eBooks+
Abdominal contour surgeries and abdominoplasty are commonly requested procedures for many reasons, including the concerns of an aging population determined to maintain a youthful physique, women intent on restoring their pre-pregnancy appearance, the rise in massive weight loss patients who are seeking to remove the stigmata of residual excess skin from weight loss, and the enhancement of self-esteem due to the implicit correlation with the appearance of a person’s abdomen and its association with health and fitness. Indeed, for many patients, the appearance and the girth of the abdomen represents a proxy for their health, fitness, and body weight.
Abdominal contour surgery constitutes a variety of procedures aimed at the aesthetic improvement of the treatable soft-tissue layers of skin, fat, and muscle ( Table 27.1 ) that impact the patient’s appearance. The goal is a firmer, flatter, more youthful-appearing abdomen through the least conspicuous and most hidden scar feasible. Depending on the anatomic nature of the “disagreeable biologic condition”, these goals can be achieved through a range of procedures referred to as the abdominolipoplasty system of classification and treatment. These procedures include liposuction alone (type I), the limited abdominoplasties – mini-abdominoplasty (type II), modified abdominoplasty (type III), and a full standard abdominoplasty (type IV) with liposuction (lipoabdominoplasty) or without liposuction of the flap ( Fig. 27.1 ). The indications for abdominoplasty are excess upper or lower abdominal skin with or without lipodystrophy and rectus muscle diastasis.
| Type | Skin | Fat | Musculofacial system | Treatment |
|---|---|---|---|---|
| I | Minimal laxity | Variable | Minimal diastasis | Suction-assisted lipectomy |
| II | Mild laxity | Variable | Lower diastasis | Mini-abdominoplasty |
| III | Moderate laxity | Variable | Lower ± upper diastasis | Modified abdominoplasty |
| IV | Severe laxity | Variable | Complete upper and lower diastasis | Standard abdominoplasty with or without suction lipectomy |
 or without liposuction. E , Excision; SAL , suction-assisted lipectomy; U , undermining.")
The anatomic boundaries of the abdomen that an abdominoplasty treats generally span from the anterior superior iliac spine to anterior superior iliac spine (ASIS) and from inframammary to pubic area. Abdominoplasty patients may request additional contouring of the flank via liposuction or flank skin excision, known as a 270° lift (or flankplasty), or completely around the entire trunk and posterior aspects, referred to as a circumferential lift or 360° liposuction. Fleur-de-lis abdominoplasty, reverse abdominoplasty, high-definition abdominoplasty, high lateral tension abdominoplasty, and bariatric plastic surgery are among the other abdominal procedures utilized.
This chapter will provide a conspectus on abdominal contour surgery and focus on abdominoplasty alone or abdominoplasty with liposuction (lipoabdominoplasty) (see Table 27.1 ), as seen in the most frequently encountered scenario of the postpartum patient.
The female abdomen undergoes the inevitable changes that all people do as a consequence of aging, weight fluctuations, and sun damage, in addition to the profound and inevitable changes from pregnancy. These issues manifest themselves as loose, damaged, and excess skin, rectus muscle diastasis and stretching, lipodystrophy, widened bony pelvic girth, potentially umbilical hernias and umbilical skin damage, and mons pubic alteration with distortion, widening, and ptosis. A full abdominoplasty is the procedure that most comprehensively addresses these changes. It can be supplemented with flap liposuction, additional skin removal, hernia repair or adjacent liposuction, as well as other unrelated aesthetic procedures.
Patients are examined and classified based on their anatomy and assigned to the appropriate abdominolipoplasty classification and treatment type ( Fig. 27.1 ). Their physical characteristics are assessed, and this information is reconciled with their tolerance for incisions, discomfort, healing time, cost, and so forth. They are offered the abdominal contour procedure most suitable to their anatomic needs and preferences. It cannot be overemphasized enough that if they choose a less-invasive or non-surgical procedures, a concept referred to as “downstaging”, although associated with less operative time, faster recovery, and lower costs, those operations do not provide the equivalent outcome of a full abdominoplasty.
Anatomic conditions that contribute to a patient’s appearance and are not improved with abdominoplasty, such as intra-abdominal fat, skeletal or spinal disfigurement, uterine malposition, and gastrointestinal dysfunction, such as bloating or distention, should be discussed and clearly conveyed to the patient. Furthermore, the surgeon should consider if the operation proposed addresses the concerns of the patient: that is, do the expectations coincide with the anticipated outcome, and if it can be determined, if the patient will be pleased with the result, “managing the patient’s expectations” is an important component of all aesthetic surgery.
Richter has summarized the pertinent anatomy of the anterior abdominal wall. Preservation of the vascular anatomy is an important factor in providing protection from skin ischemia, particularly when liposuction is performed. Lymphatic drainage of the abdominal wall infra-umbilically passes in sub-Scarpa’s plane, explaining the rationale for Scarpa’s fascia preservation and its potential reduction in seroma formation. Finally, knowledge of the innervation patterns assists in nerve blocks (i.e., TAP, Exparel [Pacira Pharmaceuticals, Parsippany, NJ], and pain pumps) for pain control and also for avoiding nerve entrapment syndromes (see Complications section below).
Preoperative preparation begins from the time of the initial consultation, and is a multidimensional process based on a series of conversations with the physician, the staff, the anesthesiologist, ancillary personnel, and the patient.
Patients receive an extensive informational brochure at the time of the consultation. Prior to surgery, they receive another detailed package outlining the preparation for surgery and the postoperative process. This includes a comprehensive list of products that adversely affect coagulation that are to be discontinued, including all non-essential supplements and over-the-counter products. For all abdominal contour surgery procedures, patients are instructed to cease nicotine-containing products and compounds that affect clotting, including hormones, for two to four weeks prior to the procedure. All patients are evaluated by a primary care physician or a specialist when indicated and undergo appropriate diagnostic laboratory tests. A history of non-IVF-related miscarriages can be a marker for these hypercoagulable conditions and that requires evaluation. Consideration is given to obtaining “special” hematology testing for genetic prothrombogenic clotting factors because patients who have these are at a considerable increased risk for blood clots. Friedman et al . offer an excellent historical battery for routine screening of hereditary thrombophilias such as protein-C deficiency, protein-S deficiency, factor V Leiden mutation or prothrombin 20210 A mutation ( Box 27.1 ). Furthermore, with the advent of COVID-19, patients post convalescence have been noted to be in a hypercoagulable state for many weeks. All patients, including fully vaccinated ones, are PCR tested as close as possible to surgery, and then quarantined before and after surgery to prevent the systemic impact of COVID-19 on a perioperative patient. Recommendations are evolving, but currently surgery should be delayed for 6 weeks after vaccines and any SARS-COVID infection, and then D-dimer testing is done to determine the patient’s coagulability prior to surgery.
Personal history of VTE (including during pregnancy or while taking oral contraceptives). Unusual site of thrombosis (mesenteric, splenic, portal, hepatic, cerebral) also increases suspicion.
Personal history of idiopathic, migratory, or recurrent SVT in the absence of varicose veins.
Personal or family history of skin necrosis when receiving warfarin. Warfarin decreases the level of natural anticoagulants, rendering the patient temporarily hypercoaguable. Development of skin necrosis is suggestive of pre-existing protein C or protein S deficiency.
Personal history of adverse pregnancy outcomes, including consecutive spontaneous abortions later than 10 weeks of gestation, three non-consecutive spontaneous abortions, severe unexplained intrauterine growth restriction, intrauterine fetal death, placental abruption, or severe preeclampsia.
First-degree relative who had a VTE, especially at a young age.
First-degree relative with known hereditary coagulopathy.
First-degree relative of a neonate with purpura fulminans without sepsis. This suggests a homozygous state of protein C and protein S deficiencies.
Professional medical photographs of all proposed surgical sites are obtained in black and white and in color.
Patients begin antimicrobial skin washes 3 days preoperatively, extending above and beyond the surgical site, including the umbilicus and perineum. Intranasal antibiotic ointment also begins preoperatively. No shaving of body hair is performed. Broad-spectrum perioperative oral and intravenous antibiotics are employed and may be continued until any drains are removed. However, evidence-based SCIP information (Surgical Care Improvement Project and prevention of postoperative infection, including surgical site infection), which confirms that antibiotics may reduce surgical site infections in abdominoplasty, also suggests that antibiotics be discontinued within 24 hours after completion of surgery.
The ERAS (enhanced recovery after surgery) perioperative principles have been advised in complicated inpatient surgeries but not validated for outpatient surgery. They can be instituted for perioperative care programs to improve outcomes after major surgery.
Preoperatively, the operating room table is checked to verify that it can reach a maximum beach chair flexed position, which is needed in order to remove the old umbilical site and is necessary for final wound closure ( Fig. 27.2 ). In the operating room, the arms are symmetrically placed on arm boards while avoiding pressure points and secured with Kerlix wraps. The patient should be kept normothermic and fluid status should be monitored. A Foley catheter is inserted for all open abdominal contour procedures and removed when appropriate, which can be before or after discharge. Abdominoplasty is performed as an outpatient procedure and it is the last operation performed in a multi-surgical operation (e.g., breast surgery, liposuction, etc.). Postoperatively, the patient is transferred to a stretcher that can achieve maximum flexion.

The modern history of abdominoplasty can be traced back to the late 1960s and the contribution of several surgeons. These procedures have evolved into the present-day abdominal contour surgery owing to the advances in technique (e.g., incision design, muscle treatment), technology (e.g., liposuction techniques), a changing population (e.g., massive weight loss), a better understanding of physiology (e.g., wetting solutions), and anatomy (e.g., the ability to do combined procedures and flap liposuction). Similar to most scientific advances, in abdominoplasty these strides have been incremental. Numerous surgeons have provided contributions to present-day abdominoplasty surgery. Table 27.2 offers a brief and incomplete overview of milestones and abdominoplasty evolution.
| Time period | Milestone |
|---|---|
| 1960s–1970s | Pitanguy, Regnault, Grazar: Classic abdominoplasty |
| 1982 | Illouz: Introduction of SAL |
| 1987 | Greminger, Noone, Wilkinson, and Hakme: Mini-abdominoplasty with liposuction |
| 1988 | Matarasso, Psilakis: Abdominoplasty system of classification and treatment |
| 1991 | Matarasso: Liposuction as an adjunct to full abdominoplasty |
| 1992 | Illouz: Abdominoplasty “mesh undermining”, marriage abdominoplasty (Shestak – 1999) |
| 1995 |
|
| 2001 | Hakme, Avelar, Saldahina, De Souza Pinto, Saltz: Liposuction |
| 2000s | Rise in bariatric plastic surgery |
| Late 2010s | Persing/others: Validation studies of lipoabdominoplasty and measures to improve safety and recommendation regarding DVT/PE |
| 2012 | Pannuci, et al ., ASPS VTE Task Force, Eric Swanson, etc. VTE prophylaxis |
| 2017 | Janis, Pollack, et al . Seroma prevention, quilting sutures |
| 2020 | Hoyos: High-definition liposuction and abdominoplasty |
Informed consent is a spectrum of patient education from the time of the initial contact with the office and until the time of surgery. Informed consent is based on the concepts that patients have the capacity to make a decision and the patient is adequately informed without coercion. Ideally it is obtained in an appropriate stress-free environment. The actual informed consent documents consist of the surgical facility’s form, the surgeon’s consent form, and an anesthesia consent obtained by the anesthesiologist. The patient, staff, and surgeon should discuss the course of treatment, the procedure, including risks, benefits, alternatives, which include not operating, financial policy, and obligations (including the financial burden of additional procedures or cancellation of scheduled surgery for non-medical reasons), and the complications in a manner that the patient understands. All interactions with the patient by telephone, text, emails, photographs, etc., should be dated, documented, HIPPA (Health Insurance Portability and Accountability Act) protected, and entered into the patient’s medical record. While a surgeon may perform the procedure numerous times, patients typically only have it performed once. Consequently, each patient deserves a thorough discussion regarding the procedure. As Nahai has stated, what is acceptable risk for one may not be acceptable risk for another.
While there are multiple local and systemic complications, untoward sequelae (conditions that resolve on their own or with minimal intervention) and nuisances, the dissatisfied patient can represent a challenging situation. Despite many publications and warning signs, it is not always feasible to know who will be dissatisfied or, conversely, who will be satisfied, until postoperatively. A general rule for aesthetic surgery is to determine preoperatively if the operation coincides with what disturbs the patient, and if, in your interactions with the patient, you believe that they will be satisfied with the outcome prior to operating. It is foolish for the surgeon to believe that they can change most patients’ personality or behavior by performing a good operation or their sincere concern for the welfare of the patient. The threshold for patient dissatisfaction seems to be lower than in years past when the truly aggrieved patient might complain to the office or file a legal action. Currently, patients do not hesitate to air any level of grievance publicly on social media. With the availability of the internet and social media, patients readily vocalize their thoughts, which can create meaningful and potentially egregious damage to the surgeon, their practice, and reputation. Management of social media in general and a dissatisfied patient (the subject of Chapter 1 ) has spawned an industry dealing with reputation management.
A well-regarded aphorism in plastic surgery is that preoperative discussions are considered an explanation, and postoperatively they are considered an excuse. The challenge with a dissatisfied or unhappy patient in aesthetic surgery is the principle that the outcome of surgery is not objectively quantifiable. Rather, it is based on their perception of the result. It might be akin to a baseball batter (patient) deciding if the pitcher’s pitch (surgeon) is a ball or strike and then, if the pitcher complains, they are penalized on social media! The patient’s opinion is influenced by a myriad of factors, such as the perioperative experience and external elements, including what their significant others feel about the result, friends, monetary issues, personal life happiness, relationships, etc. Therefore, postoperatively, “Talk therapy” management becomes the equivalent in cosmetic surgery to what occupational/physical therapy is to the outcome of hand surgery, an integral part of the surgical rehabilitation outcome. The “ripple effect” refers to how a bad experience in one aspect of the process can taint even other aspects that are essentially normal.
It is useful to inform patients that in the event that they should require reconstruction after breast cancer, an abdominoplasty will remove an important source of autologous tissue (Scott Spear, personal communication).
As noted, patients receive a detailed package of both pre-and postoperative instructions prior to the surgery. The staff, the surgeon, and the anesthesiologist call the patient and review the process prior to surgery. A history and physical examination is done with particular attention to medications, allergies, prior surgical and family history, bleeding, or clotting disorders, cardiac and pulmonary status, and scars, as well as any information that can be obtained that will improve the safety, comfort (i.e., nausea and vomiting), and outcome of the patient experience. A report is also generated by the primary care physician and is necessary for preoperative clearance. Routine chest radiographs, an electrocardiogram, and laboratory data are obtained. Any abnormalities are identified and addressed. For example, an elevated PTT (partial thromboplastin time) is most commonly due to a factor XI deficiency (Rosenthal’s syndrome). Normotensive blood pressure, less than 130 mm Hg, is necessary since hypertension is often identified as the etiology of hematoma occurrence. We also offer and encourage testing for coagulopathies. Medical consultants are liberally used for patient management.
Intraoperatively, a coordinated operating room team is essential to the smooth and safe flow of the operation. After recovery room discharge criteria are met, patients are observed overnight in an apartment-type hotel facility with experienced nurses who are versed in the postoperative management of abdominoplasty patients, including drains, Foley catheters, body movement, ambulation, diet, pain control, and bowel function. The office has regular contact and visits with the patient throughout the immediate postoperative period.
Pulmonary thromboembolism is a paramount concern, and the methods described herein are utilized. Any potential findings or symptoms described by the patient for 6 weeks or more postoperatively that are suggestive of blood clots are promptly and thoroughly investigated. Moreover, the patients are encouraged to consider having weekly postoperative venous Doppler tests of the extremities, screening for any blood clots.
Multimodal anesthesia for pain management pre-, post-, and intraoperatively is useful. In particular, setting patient expectations in terms of pain is part of that process. In addition to discomfort, pain can lead to a series of adverse side effects that begins a cascade of events that can lead to significant complications. Pain medications can cause ileus or constipation, which causes straining with bowel movements, or nausea and vomiting, which can also lead to postoperative bleeding. Moreover, pain can also reduce ambulation, which increases the risk of pulmonary thromboembolism. It also can decrease respiratory function and coughing, which can worsen atelectasis and pulmonary function.
Postoperatively, drains and sutures are removed sequentially as indicated. Generally, that is when they reach approximately 30 mL over a 24-hour period per drain, and as the color changes to become more serous in appearance. Patients should then be periodically evaluated when the drains have been removed for the presence of a seroma so that this does not lead to other sequelae, including persistent abdominal disfigurement due to a pseudobursa. We encourage intake of electrolyte-containing fluids. And, we no longer delay resumption of diet until bowel sounds are present.
A common concern of patients is when they can resume normal exercise. This is variable and not prescriptive. Exercise should begin gradually, and is based upon the type of exercise the patient wishes to engage in. This might begin at postoperative day 15–20, as circumstances dictate, initially recommending less than their normal amount of exercise and then waiting a day to observe their response before their next exercise session, then progressing as tolerated.
Another frequently asked question is: how long will healing take? Healing includes the overall appearance, absence of swelling and paresthesias, appearance of the scar, and when they can resume work and activity, among other things. All of these events occur gradually and at different and overlapping rates in each individual, and therefore cannot be accurately pinpointed. These represent a spectrum of events that occur over a period of time. Strong patient support is useful as patients progress through the postoperative period, and can be challenging, particularly with a myriad of sources, information, desire for immediate gratification, and expectations that patients have. In aesthetic surgery, “Talk therapy” is an integral component of managing patients’ results.
There may be a fine line between absolute contraindications and those that are relative contraindications to abdominoplasty. Most surgeons consider smoking and significant cardiopulmonary disease as contraindications. Complications increase with elevated body mass index (BMI) (100% over 35) and in patients with large vessel disease (which can increase infection or healing issues). Relative contraindications may be determined by the circumstances and adjudicated according to the surgeon’s experience, judgment, and risk tolerance. Age, per se , is not an absolute contraindication but the frailty index can be used to assess each individual situation. Relative contraindications include cardiac, pulmonary, and hematologic issues that impact the safety of the operation, uncontrolled hypertension, and systemic diseases, i.e., adult-onset diabetes mellitus, autoimmune diseases, and inflammatory bowel disorders. Pre-existing scars and upper, non-midline scars, i.e., a chevron/or gallbladder incision that disrupts the crossover blood supply to the distal flap when it is advanced below the umbilicus, are also issues. In these circumstances of non-midline scars, when choosing to proceed, a safety concept can be to perform it only in patients where the abdominoplasty can be closed without undermining beyond the scar or the scar can be incorporated into a vertical excision. Performing a delay of the flap first, has also been reported.
The Davison–Caprini risk stratification system for thromboembolism potential is calculated routinely preoperatively and is used as a validated risk factor modification principle. If the score exceeds 7–8 points and one elects to proceed with surgery, the patients are treated with low-molecular-weight heparin or enoxaparin sodium (Lovenox, Sanofi-Aventis, Bridgewater, NJ). Some surgeons prefer oral anticoagulation. The scale is extrapolated from inpatient general surgery patients and is not wholly transmittable to ambulatory abdominoplasty patients. Furthermore, there are various opinions as to the exact timing of the drug administration (pre-, intra-, or when to begin this postoperatively), the dose, and the duration of therapy. Our preference is to recommend preoperative testing for thrombogenic factors because of the impact positive results have on increasing the risk.
Additionally, we do not advise applying the abdominal binder until postoperative day 3 (O. Garcia, personal communication) to diminish abdominal compartment pressure, which can theoretically increase deep vein thrombosis (DVT) formation. There is a paucity of data supporting the benefits of postoperative compression garments on the wound. Ostensibly they are used to decrease fluid collection, improve scar formation, reduce postoperative edema and ecchymosis, or reduce pain. However, binders may affect pulmonary function (such as no effect or decrease), increase venous stasis, or tissue ischemia. However, in circumstances of concomitant adjacent liposuction with the abdominoplasty, the binder is applied that day. Intraoperatively, compression stockings and sequential pneumatic compression devices are always applied, and the patient’s legs are periodically flexed intraoperatively. Postoperatively, ambulation and frequent joint movement exercises are encouraged.
Body dysmorphic syndrome (and possibly borderline personality disorder) is an absolute contraindication to surgery. It has certain characteristic features and has been estimated to occur in up to 10% of plastic surgery patients (Mark Constantian, personal communication). These patients are frequently never satisfied with the results of their surgery. Plastic surgeons encounter a myriad of patient personalities and potential psychological disorders (i.e., general anxiety disorder, narcissistic personality) which may not be evident preoperatively in these patients having elective, non-essential, personal choice surgery.
Patients can get pregnant after an abdominoplasty, but some of the benefits of surgery will be lost. Our preference in patients anticipating a relatively imminent pregnancy or if a defined window of time for fertility exists, is to delay a full abdominoplasty. Patients are offered liposuction surgery as an alternative if that can achieve satisfactory results in the interim.
Smoking and nicotine products (i.e., vaping, e-cigarettes, etc.) are absolute contraindications to surgery. Our preference is that patients cease their use for a minimum of 2 and up to 4 weeks preoperatively and postoperatively.
Female and male hormones (including patches, pills, drug-eluting intrauterine devices, etc.) should be stopped due to the potential for interfering with blood clotting, and preferably for 1-month pre- and postoperatively.
All vitamins, nutritional supplements, over-the-counter products, or medications that can safely be stopped, should be discontinued approximately 2–4 weeks prior to surgery.
Medications that are deemed necessary should be evaluated on an individual basis by the surgeon, primary care/clearing physician, and anesthesiologist to determine their continued use. Recommendations are also made about future utilization, including their use on the morning of surgery (i.e., blood pressure and thyroid medications are taken the morning of surgery) and when to resume them postoperatively.
The operating table must be checked so that it reaches maximal flexed beach chair position required to consistently remove the old umbilical site. The procedure begins with injection of local anesthetic (1 mL of 1 : 100,000 epinephrine and 200 mL of 1% lidocaine in a liter of Ringer’s lactate +10 cc of transexamic acid) in the supine position with the abdomen minimally hyperextended, so that the injection needle stays tangential, thereby avoiding its inadvertent peritoneal cavity penetration. The patient is then turned to the prone position by a coordinated team effort led by the anesthesiologist and surgeon if other planned treatment sites are better accessed in that manner. Those posterior sites are then injected with local anesthetic, prepped, and draped and operated upon. When higher doses of local anesthetic become necessary, sequential injections are performed in order to avoid excessive doses of superwet injectate. For the abdomen itself, we rarely exceed 1 liter of injectate because it is unnecessary, and any excess fluid impedes electrocoagulation. This also allows more injectate to be safely used in other areas.
Not all postoperative concerns represent complications. A distinction should be made between a revision , such as the need to correct a complication, unsatisfactory result, or for further improvement that may not have been feasible, recognized, or necessary at the initial operation, and secondary surgery on another surgeon’s patient. For example, dog-ears, despite appropriate planning and wound closure, can be inevitable consequences of the disparity created by upper abdominal dissection that changes the symmetry of the upper and lower excisions, and also the fact that a standard abdominoplasty is only treating 180° of a 360° structure. If dog-ears occur, we endeavor to have the patient agree to wait some months prior to revision so that the wound can contract. Superficial liposuction and steroid injections can sometimes improve minimal excess tissue. Those that do not resolve require revision.
Untoward sequelae include those things that resolve spontaneously or with minimal intervention over time. These include hypesthesias, paresthesias, feelings of tightness, intermittent episodes of feelings of swelling or enlargement, bruising, edema, mons pubis swelling or scrotal enlargement. Refractory hypesthesias and uncomfortable pruritic itching can be particularly irritating and have been successfully treated with Lyrica (Viatris Inc., Canonsburg, PA). Scars mature over a lengthy period of time, and counseling about the role of scar products (gels, tapes, etc.), the use of energy devices to modify them, triamcinolone acetonide injections, and avoiding sun and smoke exposure are useful as the body undergoes the natural healing process. During periods of sunbathing, patients should avoid using dark clothing until full sensation returns, as the diminished skin sensation can result in a burn.
No surgeon begins an operation expecting a complication. These can be particularly distressing in elective, healthy patients undergoing non-essential cosmetic surgery. In complications that are not resolved quickly (i.e., hematomas), such as wound healing problems (i.e., necrosis) that can take long periods of time to resolve, patients’ access to things like search engines, social media, etc., can be deleterious to the trust that is necessary for the important doctor–patient relationship needed to resolve the problem and thus can exacerbate an already difficult scenario.
Awareness and incorporating steps to potentially avoid complications can help reduce, but not eliminate, their occurrence. Numerous databases reporting complications exist. These include: the American Society of Plastic Surgeons (ASPS) TOPS registries (Tracking Operations and Outcomes for Plastic Surgeons) and The Doctors Company data (TDC), American College of Surgeons NSQIP (National Surgical Quality Improvement Program), CosmetAssure, American Board of Plastic Surgery (ABPS) tracer data for continuous certification, AAAASF (American Association for Accreditation of Ambulatory Surgery Facilities), surveys, and individual surgeon reports. Complications can be subdivided into local versus systemic, early versus late, or by the type of abdominal contouring surgery that is performed ( Box 27.2 , Tables 27.3–27.6 ). In the final analysis, it is essential to bear in mind, that because of the way sources capture their data, that the risk factors identified and the complications reported can be different.
Case series reports of a surgeon.
Surveys of groups of plastic surgeons (e.g., American Society of Plastic Surgeons, American Society for Aesthetic Plastic Surgeons, etc.)
TOPS (Tracking Operations and Outcomes for Plastic Surgery): National database of plastic surgery procedures and outcomes self-reported by members of American Society of Plastic Surgeons.
CosmetAssure: A medical insurance program covering 17 elective cosmetic procedures performed by active or candidate members of the American Society of Plastics Surgeons. Coverage includes complications treated in an emergency room, those requiring hospital admission, or intervention in an accredited surgical center within 30 days of the procedure. It does not include complications treated on an outpatient basis, such as seroma drainage, wound care, or oral antibiotics, which TOPS should include.
The Doctors Insurance Company: Data based on claims that the insured physician's medical malpractice covers.
Maintenance of Certification (MOC – now Continuous Certification): Data collected by the American Board of Plastic Surgeons for board certification.
American Association for Accreditation of Ambulatory Surgical Facilities (AAAASF): Data collected from outpatient accredited surgery centers.
American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) – is risk adjusted and tracks patients for 30 days after their operation.
| Complication | % |
|---|---|
| Infection | 1.63 |
| Hemorrhage | 1.17 |
| Fluid overload | 0.33 |
| R/O DVT b | 0.3 |
| Hypoxia | 0.24 |
| Pulmonary dysfunction | 0.22 |
| R/O PE b | 0.22 |
| PE | 0.19 |
| Severe hypertension | 0.16 |
| DVT | 0.16 |
| Overall R/O rate of abdominoplasties | 4.7 |
| Overal R/O rate of other cosmetic procedures | 1.37 |
a Abdominoplasty alone 37%; abdominoplasty with multiple procedures 67%.
b About half of suspected DVTs were DVTs; almost all suspected PEs were positive.
| Complications | Liposuction (%) | Limited abdominoplasties (%) | Full abdominoplasties (%) |
|---|---|---|---|
| Contour irregularity | 9.2 | 4.9 | 5 |
| Major skin necrosis (requiring re-operation) | 0 | 1 | 1 |
| Minor skin necrosis (healed spontaneously) | 0 | 4 | 4.4 |
| Scar revision | 0.03 | 2.4 | 4.9 |
| Hematoma | 0.04 | 0.08 | 1.4 |
| Wound infection | 1 | 0.02 | 1.1 |
| Wound dehiscence | 0 | 1 | 1 |
| Umbilical abnormality (requiring re-operation) | 0 | 0.05 | 1.2 |
| Dissatisfied patient (unfulfilled expectations) | 3.3 | 2.9 | 2.2 |
| Need for second surgery | 3.5 | 2.4 | 3.4 |
| Complications | Liposuction | Limited abdominoplasties (%) | Full abdominoplasties (%) |
|---|---|---|---|
| Local anesthesia (i.e., wetting solution) | 0 | 0 | 0 |
| Major anesthesia | 0 | 0 | 0 |
| Malpractice action | 0 | 0 | 0.01 |
| Blood transfusion | 0 | 0 | 0.04 |
| Deep vein thrombophlebitis | 0 | 0.01 | 0.04 |
| Pulmonary embolism | 0 | 0 | 0.02 |
| Intra-abdominal perforation | 0 | 0 | 0 |
| Death | 0 | 0 | 0 |
| Readmission to hospital | 0.01 | 0.01 | 0.05 |
| Complication | Matarasso et al. , 2006 | Hester et al ., 1989 | Grazer and Goldwyn, 1977 | Pitanguy, 1983 | Teimourian and Rogers, 1989 |
|---|---|---|---|---|---|
| No. of procedures | 11,016 | 563 | 10,490 | 539 | 25,562 |
| Local (%) complications | |||||
| Necrosis minor | 4.4 | 0.9 (minimal slough) | 5.4 (wound dehiscence) | 1.4 | |
| Necrosis major | 1 | 0.3 | |||
| Seroma | 2.5 | 5.8 | 8.58 | ||
| Infection | 1.1 | 1.1 | 7.3 | ||
| Blood loss | <1.0 | 14.2 | |||
| Hypertrophic scars | <1.0 | 3.7 | |||
| Hematoma | 1.4 | 6 | |||
| Wound infection | 1 | ||||
| Dehiscence | 1 | 0.3 | |||
| Umbilical abnormality | 1.2 | 0.3 | |||
| Dissatisfied patient | 2.2 | ||||
| Need for second operation | 3.4 | ||||
| Scar revision | 4.9 | ||||
| Contour irregularity | 5 | ||||
| Systemic (%) complications | |||||
| Deep vein thrombosis | 0.04 | 1.1 | 0.29 | ||
| Pulmonary embolism | 0.02 | 1.1 | 0.8 | 0.25 | |
| Pulmonary fat embolism | 0 | 0.02 | |||
| Blood transfusion | 0.04 | 0.04 | |||
| Death | 0 | 0.16 | 0.04 | ||
| Anesthesia complications | 0 | 0.01 | |||
| Readmission to hospital | 0.05 | ||||
| Malpractice action | 0.01 | 0.18 | |||
Traditionally, pulmonary atelectasis or seromas were considered the most common complications reported. However, because of how certain databases draw their information, these may not even be listed.
CosmetAssure data reveal that there is an overall 4% complication rate for abdominoplasty (of which 31.5% were hematomas, 27.2% were infections, and 20.2% were suspected or confirmed venous thromboembolism [VTE]) versus 1.4% for all other aesthetic surgery (see Table 27.3 ). Risk factors include male sex, age greater than 55 years, BMI greater or equal to 30, combined procedures (abdominoplasty alone was 3.1%, with liposuction increased to 3.89%, with breast surgery to 4.3%, with liposuction and breast surgery to 4.6%, with body contour surgery to 6.8%, and highest in abdominoplasty with liposuction and body contour surgery at 10.4%) It was also reported to be higher in a hospital or surgicenter than in an office-based surgery suite. In terms of DVT risk, abdominoplasty was 0.5% and increased to 1.1% in liposuction and abdominoplasty.
Perhaps due to the fact that this database looks at complications requiring return to the operating room within 30 days postoperatively, seromas and pulmonary atelectasis are not listed here as a complication and smoking is not included as a risk factor.
ASPS–TOPS data report infection being the most common complication (3%–5%).
ABPS continuous certification data report infections followed by seromas, and venous thromboembolism as the most frequent.
Infections are often considered the second most common complication of an abdominoplasty, occurring at a rate of 1%–3.8%. Risk factors include obesity, smoking, diabetes, malnutrition, and an immunosuppressed state. Signs and symptoms include erythema, inflammation, edema, tenderness, elevated temperature, elevated white blood cell (WBC) count and possibly systemic symptoms. Skin flora account for the majority of infections (but can also include anaerobes and atypical mycobacteria). For prophylaxis, patients are instructed to begin antimicrobial skin washes three days preoperatively and are given intranasal antibiotic ointments and perioperative antibiotics until the drains are removed. The field is widely prepped with alcohol-containing solution, with the perineum cleansed last. The umbilicus is further decontaminated with a betadine-soaked applicator. Intraoperatively, in an effort to reduce infection, the patient is kept normothermic, the surgical field is irrigated with saline prior to closure, and the drains are soaked in a betadine solution before their placement. In the postoperative period, the abdomen is inspected for signs and symptoms of infection. If infection is confirmed, drains should be removed when possible. Depending on the degree of concern about an infection, the wound is explored, copiously irrigated, cultured (including Mycobacterium and anaerobes), so the appropriate antibiotic coverage can be instituted, beginning with the result of the Gram stain report.
Rapidly progressing and erythematous-appearing wounds warrant the consideration that they may represent necrotizing fasciitis and immediate treatment should be instituted.
Fluid collections include seromas and hematomas or possibly an infection. Seromas represent the most common local complication (although atelectasis can occur more frequently in up to 40% of patients). Abdominoplasty carries a high risk of seroma formation. These are multifaceted in etiology and can range from a trivial nuisance to an untoward sequelae, to the formation of pseudobursas. Various strategies have been suggested to reduce seroma formation, including avoiding flap dissection with electrocautery, preserving fibrous tissue on the rectus fascia, preserving Scarpa’s fascia, not using binders (to prevent shearing of the tissue layers), using tissue sealants, glue, drains, and/or progressive tension sutures, avoiding overhydration, and adding a weak diuretic (hydrochlorothiazide 25 mg orally for 1 month). Interestingly, some have even suggested that lipoabdominoplasty reduces the risk of seroma formation.
In limited abdominoplasties, we place one drain; in full abdominoplasty two Jackson–Pratt drains; and in massive weight loss patients four drains. We have recently begun using a four-drain Interi System VAC device for drainage (IC Surgical, Grand Rapids, MI) with satisfactory preliminary results in terms of reducing seromas and enhancing wound healing. It is considered an internal negative-pressure delivery system. Drains are removed when the color becomes more serous in appearance and the volume is less than 30–40 mL over a 24-hour period. They can be kept in place for days and occasionally for so long due to a higher than ideal output that the surgeon is pressed to make a clinical judgment about the timing of their removal. Drain management by various apps, as well as patient–nurse education, are valuable in achieving optimal utilization of the drains.
Numerous authors have described other methods to limit fluid collection after an abdominoplasty. Progressive tension sutures, alone or in combination with drains, have proven to be safe and effective in reducing dead space and decreasing seroma formation. Surgeon preference, experience, and technique ultimately dictate the use of drains, glue, progressive tension sutures (PTS), or a combination in order to reduce dead space and fluid accumulation.
Referring, however, to progressive tension sutures as a distinct operation procedure known as “drainless abdominoplasty” is a misnomer. Rather, it simply represents a technical variation and a method of reducing fluid collections. When using progressive tension sutures, care should be taken not to take too deep a suture bite on the abdominal surfaces, initiating a nerve entrapment syndrome. Deep bites in the undersurface of the flap, creating surface contour irregularities, tend to resolve over time.
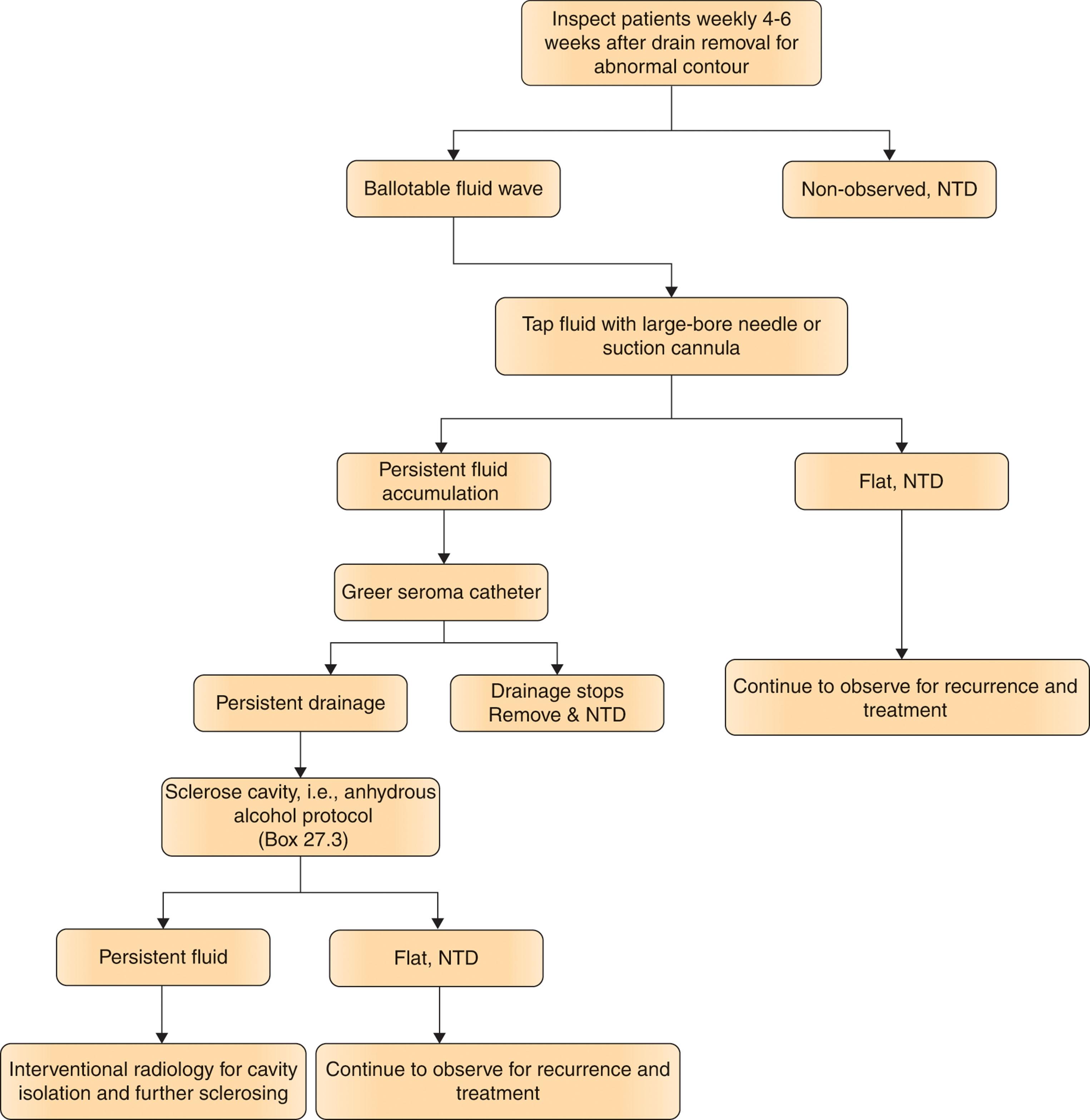
Once drains are removed, seromas can be identified in the early postoperative period by a ballotable fluid wave and should be treated to avoid potential sequelae, such as infection, toxic shock syndrome, or pseudobursas. They are initially managed by serial aspiration using a large-bore needle or a liposuction cannula. If they persist, a seroma catheter can be placed. Continued drainage can be treated by sclerosing, using anhydrous alcohol by the surgeon, or by an interventional radiologist localizing it, and then insertion of pigtail catheters, and sclerosing. ( Box 27.3 , Algorithm 27.1 ). Persistent seromas can result in a visible surface contour irregularity from pseudobursas, which generally have to be surgically excised.
Suction out area via wall suction to ensure no fluid present in cavity prior to instilling anhydrous alcohol.
Using a sterile JP drain soaked in povidone-iodine (Betadine) secure beneath soft tissue in sterile fashion.
Draw up 3 mL of anhydrous alcohol in Luer-Lok syringe and attach syringe to end of clamped drain tube.
Unclamp drain tube and inject 3 mL into the tubing and clamp right after. Wait 5–10 minutes to assess patient’s tolerance.
If tolerated, proceed to use 25 mL of anhydrous alcohol and inject into unclamped tube and, once injected, clamp tubing and keep in place for next 30 minutes.
After 30 minutes, use wall suctioning, attach end of drain tube to suction tube to remove any residual fluid.
Abdominoplasty surgery does not usually result in significant amounts of blood loss. Larger volumes of blood loss in abdominoplasty patients can be attributed to concomitant liposuction. Blood loss from liposuction is approximately 1.9 grams of hemoglobin per 2343 mL of liposuction. Ninety-eight percent of that is third-space loss into the interstitial fluid and 1.76% of the aspirate collected is blood. The decrease of hematocrit persists to about postoperative day 7 and gradually returns over 30 days. Fluid replacement is important in patient management. It should be approximately 1:1 by hypodermoclysis (80% of injected superwet fluid is absorbed and 20% is suctioned out). Then, over the first 24 hours, another 1:1 of fluid is replaced intravenously and by oral intake. When lipoaspirate exceeds 4 L, deficit and maintenance are replaced with 0.25 mL per mL of aspirate over 4 L.
Hematomas are a common concern in all plastic surgery procedures. The reported incidence is approximately 2%. Consequently, strategies that might reduce their development are employed at every juncture. Preoperatively, patients receive an extensive list of medications that inhibit coagulation, to stop 2 weeks preoperatively and have a thorough history taken and laboratory data to assist in uncovering patients’ predisposed bleeding disorders. Intraoperatively obtaining meticulous hemostasis at regular intervals cannot be overemphasized (“red to black”). Numerous studies have shown that strictly maintaining postoperative blood pressure, preferably below 130 mm Hg, may be the most significant factor in reducing hematoma formation in all aesthetic surgery. Bear in mind when considering strategies to reduce bleeding that drains do not prevent hematomas. Also, the “second” operation for complications causes more consternation for the patient, is not usually scheduled as an elective procedure, takes longer than the first procedure, and is bloodier to perform.
Hematomas can appear in the early postoperative period or, due to the large, empty space of the abdomen, may not appear until later in the postoperative period. Consequently, signs used to identify hematomas in other operations, such as sudden enlargement, often after localized pain, edema, and ecchymosis, may not appear as early signs after an abdominoplasty. Therefore, in conjunction with the patient’s exam, observing the volume and color of drain output (which is often higher in patients who have had concomitant liposuction), or change in the appearance of the abdomen can be helpful for diagnosis.
The correct treatment for hematomas will depend on the size of the hematoma, the context of its occurrence, and the status of the patient. In contrast to a protocol that can be used for some small non-expanding facelift hematomas, bedside treatment of abdominoplasty bleeding is usually not recommended. In most situations, diagnosed abdominoplasty hematomas are larger than elsewhere. The patient should be returned to the operating room and typically the entire abdomen opened and explored. Our preference is to suction out the wound while preparing for surgery and inducing anesthesia, in order to remove the excess blood. Consequently, the wound and surgical field is clear upon opening the abdomen. The wound is then copiously irrigated with saline and then antibiotic solution. More commonly, generalized oozing, as opposed to pumping vessels, are encountered. Hemostasis is obtained using electrocautery (irrigation with 3% hydrogen peroxide may reduce bleeding also). Hemostatic agents can also be applied to the wound bed if needed. If hemostatic agents are used, the field should again be irrigated prior to drain placement to avoid clogging of the drains from them. Despite the increased potential for DVT/PE from a second anesthetic, these are situations where consideration should be given to using a binder immediately postoperatively.
When reflecting on the etiology of a hematoma or concern for recurrence, issues such as surgical technique, blood pressure spikes, and bleeding disorders should be considered. Also, males and patients who have previously had abdominal liposuction tend to be at a greater risk.
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are underdiagnosed conditions and can be devastating, life-threatening events, that occur as frequently as 1.1% of abdominoplasties and account for half or more of all abdominoplasty fatalities. Screening for and modifying high-risk situations, perioperative prophylaxis, and postoperative surveillance is essential.
Multiple factors intrinsically render abdominoplasty particularly prone to VTE. Venous stasis might be exacerbated by third spacing, increased intra-abdominal pressure, tight external compression garments, and flexed positioning that decreases venous return from the lower extremities. Other predisposing risk factors for venous thromboembolism may include vessel injury incurred secondary to intense dissection of superficial veins, decreased peripheral vascular resistance associated with general anesthesia, and decreased postoperative mobility.
Numerous risk factors unrelated to abdominoplasty in and of itself, such as length of surgery, combined procedures, smoking, obesity, family history, hereditary thrombophilias, immobilization, cardiac or pulmonary history, varicose veins, rectus muscle plication, hormones, and dehydration are just some factors that can be associated.
There is an entire expanding body of literature related to thromboembolism and abdominoplasty. Thus, a myriad of recommendation schemes exist regarding methods of minimizing VTE in surgical patients. The seventh American College of Chest Physician Consensus Conference on Antithrombotic Therapy stratified patients into four venous thromboembolism risk categories (low, moderate, high, and highest) defined by age, type of surgery, and additional risk factors. Although this report is a very important theoretical step in the direction of appropriate risk-based venous thromboembolism prophylaxis in plastic surgery, and its schema is often considered by plastic surgeons, it is not clear whether plastic surgery procedures qualify as “minor”, “non-major”, or “major”, and the system is therefore not necessarily directly generalizable to our field.
The Davison–Caprini model is a widely accepted framework for venous thromboembolism risk stratification and prophylaxis in plastic surgery. The typical abdominoplasty is rated at four points (two for “major surgery” and two for a patient older than 40 years), immediately classifying the operation as high risk. Others consider the operation itself to be worth five points.
We recommend that all patients are well hydrated and fluid status monitored, and patients wear compression stockings and sequential pneumatic compression devices. Intraoperatively, their legs are frequently flexed and massaged. Postoperatively, they ambulate in the recovery area. Incentive spirometers are used.
Pharmacologic anticoagulation has been a predominant consideration over the past decade, and there are numerous studies and proponents on both sides for and against its use. Many advocate oral or injection medications based on a risk-qualified model, such as the Venturi modification of the Davison–Caprini system to determine the need for anticoagulation and recommend it for a score greater than 7–8. When to begin it, how long to use it for, and the dosage varies. When we use enoxaparin sodium (Lovenox) we use 40 mg subcutaneously beginning 8 hours from the onset of surgery, for 3–5 days or longer if indicated due to thrombophilias. Some surgeons prefer a twice-daily weight-based protocol of 0.5 mg/kg. Although the presentation of VTE is non-specific, and often asymptomatic, surgeons must maintain a high level of clinical suspicion for VTE, because the consequences of missing a DVT are so serious. For example, it must be excluded in patients with any suggestive signs or symptoms, such as, pleuritic chest pain, positive Homan’s sign, any localized findings, shortness of breath, cardiac signs, or emotional changes.
Pulmonary embolism and pulmonary fat embolism syndrome can have overlapping signs and symptoms. They must be distinguished from each other as the treatments are different.
The American Academy of Family Physicians (AAFP) and the American College of Physicians (ACP) provide four recommendations for the workup of patients with probable DVT.
First, is the Wells clinical prediction rules to estimate and interpret the probability of VTE (this is better in younger patients without comorbidities or a history of VTE).
Second, in appropriately selected patients with low pretest probability of VTE is a high-sensitivity D-dimer test (degradation products of cross-linked fibrin by plasmin that are detected by diagnostic assays) that is elevated. Many conditions such as recent surgery, hemorrhage, cancer, trauma, or sepsis can cause an elevation. Scores can be age adjusted. They remain elevated for about 7 days and will not be high after clot organization or in small, isolated, or solitary calf vein DVT. Because it has a high sensitivity (up to 97%) and low specificity (as low as 35%) it should only be used to rule out, not confirm the diagnosis of a DVT. A negative test in Wells (DVT <2) low-to-moderate risk patients rules out DVT and further surveillance.
Third, patients with positive D-dimer tests and Wells moderate-to-high risk (Wells DVT score >2) require a diagnostic study (duplex ultrasonography).
Fourth, patients with intermediate or high pretest probability of pulmonary embolism require diagnostic imaging studies. Options include ventilation perfusion (V•/Q) scan, multidetector helical computed axial tomography (CT) and pulmonary angiography.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here