Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The function of the gastrointestinal (GI) system is to break down food for absorption into the body. This process occurs in five main phases: ingestion , fragmentation , digestion , absorption and elimination of waste products. Digestion is the process by which food is enzymatically broken down into molecules that are small enough to be absorbed into the circulation. As an example, ingested proteins are first reduced to polypeptides and then further degraded to small peptides and amino acids that can be absorbed.
The gastrointestinal system is essentially a muscular tube lined by a mucous membrane that exhibits regional variations, reflecting the changing functions of the system from mouth to anus. The mucous membrane is protective, secretory, absorptive or a combination of these in different parts of the tract (see Fig. 14.3 ). The muscle gives strength to the wall of the tract as well as moving the food along. Muscle is arranged somewhat differently in different areas of the tract. Because of its continuity with the external environment, the gastrointestinal system is a potential portal of entry for pathogenic organisms. As a result, the system incorporates a number of defence mechanisms which include prominent aggregations of lymphoid tissue, known as the gut-associated lymphoid tissue ( GALT ), distributed throughout the tract (see Ch. 11 ).
The GI tract is derived from endoderm , the innermost of the three layers forming the developing embryo. During fetal life, it is divided into three segments described as the foregut (with blood supply derived from the coeliac trunk), midgut (supplied by the superior mesenteric artery) and hindgut (supplied by the inferior mesenteric artery). These parts develop into the parts of the definitive GI tract. The foregut extends from the oesophagus down to the second part of the duodenum where the common bile duct enters the GI tract. The midgut extends to the junction of the middle and distal thirds of the transverse colon (known as Cannon’s point ), and the more distal structures are derived from the hindgut. An awareness of the embryological development of the GI tract often facilitates our understanding of disease. For example, visceral pain arising from the different parts of the gut typically localises in distinct parts of the abdomen due to the pattern of its innervation. As a result, foregut pain is typically felt in the epigastrium , midgut pain in the periumbilical region and hindgut pain in the suprapubic area. This helps explains why the pain of acute appendicitis tends to begin in the periumbilical area (midgut origin) and only localises to the right iliac fossa later because of inflammation of the peritoneal surface.
Peristalsis is the primary mechanism by which food is propelled along most of the length of the GI tract, with some voluntary muscular action involved at both extreme ends of the process. The particular anatomical arrangement of smooth muscle in the wall of the GI tract is specialised to allow constriction of the luminal diameter (via the circular layer of muscle) as well as shortening of its length (via action of the longitudinal muscle layer). The coordination of this very complex mechanism acts to progressively squeeze food along and, in certain sites such as the stomach, also facilitates churning and mixing of the food to aid digestion. The autonomic nervous system is responsible for the control of this involuntary process, primarily via parasympathetic innervation of the gut.
Certain disease states and drug treatments can interfere with the normal process of peristalsis. One uncommon condition called Hirschsprung’s disease is characterised by failure of migration of ganglion cells into the GI tract, usually in the rectum and distal colon. Patients with this disorder typically present with severe and chronic constipation and may develop progressive dilatation of the bowel. In its most extreme form, absolutely no ganglion cells are present in the bowel, and some patients develop aganglionic megacolon due to this failure of propulsion of food through the bowel.
A variety of drug treatments, including commonly using strong painkillers such as opiates, can produce severe constipation by interfering with normal peristaltic function.
A vast range of both neoplastic and non-neoplastic disorders can affect the GI tract. A ‘surgical sieve’ can be used to categorise all the potential differential diagnoses for a particular clinical presentation. For example: inflammation, infection, neoplastic (including dysplasia and invasive malignancy), metabolic, congenital, vascular, iatrogenic (including drug effects), autoimmune and trauma.
CM circular muscle layer E stratified squamous epithelium G seromucous glands LM longitudinal muscle layer LP lamina propria Ly lymphoid aggregate MM muscularis mucosae MP muscularis propria Sk skeletal muscle Sm smooth muscle SM submucosa PG parasympathetic ganglion
The importance of the physiological sphincter at the gastro-oesophageal junction is apparent when the consequences of malfunction are considered. Reflux through the sphincter allows gastric acid into the lower oesophagus, causing the well-known symptom of ‘heartburn’. With time, the epithelium of the lower oesophagus undergoes metaplasia , i.e. it converts to a columnar mucus-secreting form, a reaction that may well be protective. Barrett’s oesophagus (see e-Fig. 14.1 ) is the term given to this metaplastic columnar epithelium of the lower oesophagus. This metaplastic epithelium is at high risk of developing dysplasia and invasive adenocarcinoma. Oesophageal carcinoma generally has a poor prognosis.

The stomach is a very unique environment due to the ability of its mucosa to secrete concentrated hydrochloric acid as well as digestive proteolytic enzymes. In order to avoid mucosal damage and digestion of the stomach itself, the normal stomach also secretes a protective alkaline mucus. The balance between potentially damaging and protective factors can be disrupted in various conditions, resulting in inflammation of the stomach or gastritis . More severe mucosal damage can occur, leading to development of an ulcer (complete loss of the mucosa) or erosion (loss of part of the thickness of the mucosa). When there is excessive secretion of acid and digestive enzymes, mucosal damage may not be limited to the stomach itself but often extends into the proximal duodenum. The underlying causes of such peptic ulceration are diverse . Agents such as alcohol and drugs can lead to mucosal damage, sometimes by direct toxic effects upon the mucosa and sometimes by interfering with normal protective mechanisms (e.g. non-steroidal anti-inflammatory drugs can cause damage by inhibiting synthesis of protective prostaglandins). Infection by the organism Helicobacter pylori is a very important cause of gastritis and peptic ulceration, and the mechanism by which it causes mucosal damage is discussed later.


C circular muscle GM glandular mucosa GP gastric pit L longitudinal muscle M mucosa MM muscularis mucosae MP muscularis propria O oblique muscle SE squamous epithelium SM submucosa
Most gastric cancers are adenocarcinomas which are of either intestinal type, characterised by glandular differentiation or diffuse type, characterised by infiltrating single tumour cells such as signet ring cells. The latter results in linitis plastica or the so-called ‘leather bottle stomach’ where the tumour diffusely infiltrates the stomach wall.

B bacterium BM basement membrane C canaliculus CC chief cells E neuroendocrine cells F foveola LP lamina propria M mitochondrion MM muscularis mucosae Mu mucous cell PC parietal cell SM submucosa
Acid production by parietal cells is controlled via the autonomic nervous system and through the action of hormones. Parasympathetic innervation by branches of the vagus nerve results in release of acetylcholine , which acts on muscarinic M3 receptors on parietal cells. The hormone gastrin is produced by G cells in the antrum in response to rising gastric pH, and it acts via CCK2 receptors on the parietal cells. Histamine also increases acid secretion, acting via H2 receptors.
Stimulation of these various receptors results in activation of protein kinases, either via an increase in the concentration of intracellular calcium (in the case of muscarinic and gastrin receptors) or by increasing levels of cAMP (in the case of histamine), leading to active secretion of acid (see Fig. 14.11 ). As acid production increases, the pH in the gastric antrum falls. In response to this, the D cells in the antrum produce another hormone, somatostatin , and this acts on the antral G cells to reduce secretion of gastrin.

B Brunner’s glands CC chief cells CM circular muscle D duodenum E neuroendocrine cell G G cells LM longitudinal muscle MM muscularis mucosae P gastric pit PC parietal cell PS pyloric sphincter rER rough endoplasmic reticulum S stomach ZG zymogen granule
H. pylori infection is a major cause of gastritis and peptic ulceration. The organism does not invade the tissues but inhabits the protective mucus layer which covers the surface of the mucosa. It has a unique ability to survive the acid environment of the stomach because of a bacterial enzyme, urease . This allows it to produce ammonia by splitting urea, raising pH in the immediate vicinity of the organism. It typically colonises the antrum and, by producing a localised alkaline environment here, H. pylori interferes with normal physiological control of gastric acid secretion. The falsely high antral pH stimulates secretion of gastrin by the antral G cells, which acts upon the parietal cells in the body to increase acid production still further. This excess acid production overwhelms normal mucosal defence mechanisms, leading to the formation of an acute ulcer.
B Brunner’s glands C crypt CM circular muscle LM longitudinal muscle M mucosa MM muscularis mucosae P Peyer’s patch PC plica circularis S serosa SM submucosa V villus
Understanding of the role of H. pylori has revolutionised management of peptic ulceration. In the past, peptic ulcers were treated by surgical procedures which aimed to reduce acid production, such as partial gastrectomy (to remove the antral source of gastrin) or vagotomy and pyloroplasty (removing the vagal-driven pathway of acid secretion but requiring release of the pylorus, since the vagus nerve also controls gastric emptying). Such operations were associated with considerable morbidity.
Conventional medical management of peptic ulcer disease employed a range of drugs from simple alkalis to neutralise excess acid, through various drugs which interfere with normal physiological control of acid secretion (e.g. adrenergic antagonists and histamine (H 2 ) receptor blockers), to the more recent use of proton pump inhibitors (PPIs) which effectively block the final common pathway of acid production.
Although acid-blocking drugs were usually effective, treatment had to continue life-long. Now, treatment usually requires only a short course of Helicobacter eradication therapy, using a combination of two antibiotics with a proton pump inhibitor (‘triple therapy’).
Digestion occurs within the lumen or at the mucosal surface, where it is linked with the process of absorption.
Luminal digestion involves the mixing of chyme with pancreatic enzymes to break up foods into their component parts. The process is facilitated by adsorption of pancreatic enzymes onto the mucosal surface. Membrane digestion involves enzymes located in the luminal plasma membranes of the enterocytes. The principal means of digestion and absorption of the main food constituents are as follows:
Proteins are first denatured by the gastric acid and then hydrolysed to polypeptide fragments by the enzyme pepsin. In the duodenum, pancreatic enzymes including trypsin , chymotrypsin , elastase and carboxypeptidases continue this process, producing small peptide fragments. Membrane-bound peptide hydrolases complete the digestion to amino acids that are then absorbed. Absorption is by active transport, with a different carrier system for each amino acid. In young infants, some proteins are absorbed without prior digestion by the process of endocytosis.
Carbohydrates occur in the diet mainly in the form of starches and the disaccharides sucrose and lactose. Pancreatic amylase hydrolyses starch to glucose and the disaccharide maltose in the small intestinal lumen. This process is begun by salivary amylase in the mouth, although its contribution to digestion is probably minor. Membrane-bound disaccharidases and oligosaccharidases convert the sugars to monosaccharides, mainly glucose, galactose and fructose, which are absorbed by facilitated diffusion.
Lipids , predominantly triglycerides, are converted by the mechanical action of the stomach into a coarse emulsion which is converted to a fine emulsion in the duodenum by bile acids , synthesised in the liver. Each triglyceride molecule is broken down into a monoglyceride and two free fatty acids by pancreatic lipases, although some glycerol and diglycerides are also produced. These smaller lipid molecules are then absorbed and resynthesised back into triglycerides within the enterocytes.
Coeliac disease (or coeliac sprue or gluten-sensitive enteropathy) is caused by an immunological response to gluten ( gliadin ), a component of wheat, oats, barley and rye. Individuals with this condition present with symptoms of malabsorption, including weight loss, diarrhoea, steatorrhoea, anaemia and vitamin deficiencies. The immune response damages the small bowel mucosa, resulting in loss of the surface villi and elongation of the crypts. Blood tests reveal characteristic anti-endomysial antibodies , as well as specific antibodies against tissue transglutaminase .
")
Endoscopic biopsy of the small intestine is usually performed for diagnosis. The typical histological changes are illustrated in Fig. 14.20 . Although these histological appearances are very suggestive of coeliac disease, they are not specific and the diagnosis must be confirmed by resolution of the symptoms and histological changes after a period of time on a gluten-free diet.

C crypts CM circular muscle E enterocyte L lacteal LM longitudinal muscle LP lamina propria MM muscularis mucosae Mv microvilli PP Peyer’s patch PC plica circularis Se serosa SM submucosa V villus
C capillary G granule Go Golgi apparatus L lacteal Ly lymphocyte M mitochondrion Mu smooth muscle fibres P plasma cell R ribosomes rER rough endoplasmic reticulum V villus
BM basement membrane BM E endothelial basement membrane C capillary Ch chylomicron Co collagen fibrils En endothelium EV endocytotic vesicles F microfilaments Fi fibroblast G glycocalyx IC intercellular cleft J junctional complex LD lamina densa Ly lymphocyte M mitochondrion Mv microvilli R ribosomes sER smooth endoplasmic reticulum T microtubules TW terminal web V membranous transport vesicle
CM circular muscle E endocrine cell G goblet cell L large intestine LM longitudinal muscle Ly lymphoid tissue MF mitotic figure MM muscularis mucosae MP muscularis propria P Paneth cell S small intestine SM submucosa T T lymphocyte V villus
The colon and rectum are subject to a variety of conditions including infections, inflammatory disorders (discussed later) and vascular disorders. Acute infections often result in diarrhoea and are usually short lived. More chronic infections such as amoebic colitis and those associated with immunocompromise (e.g. cytomegalovirus) are usually diagnosed on biopsy and require special stains for confirmation.
Diverticulosis, in which the mucosa herniates through the bowel wall, can cause an acute abdomen by becoming inflamed with abscess formation or perforation. Vascular compromise of the bowel can occur as a result of herniation, embolus in the blood supply or volvulus (twisting) of the bowel wall.
Malignant tumours arising in glandular epithelium are called adenocarcinomas. Adenocarcinomas of the colon and rectum (commonly referred to as bowel cancers) are common in older patients, particularly in developed countries. This is in contrast to adenocarcinomas of the small intestine, which are comparatively rare.
Intensive research has identified a number of risk factors for the development of colorectal carcinoma, including the prior existence of benign tumours (adenomas) in the bowel, the presence of long-standing ulcerative colitis (a form of chronic inflammatory disease affecting the colon), inherited syndromes such as familial adenomatous polyposis and Gardner syndrome (in which patients have innumerable adenomas in the bowel due to a genetic abnormality) and also factors such as low dietary fibre intake.
The sequence of events involved in the development of some adenocarcinomas is becoming clearer, and it appears to require the accumulation of a number of genetic abnormalities ( mutations ), generally arising in a specific order. The acquisition of these mutations can be detected as the epithelium changes from normal to an adenoma, with increasing degrees of dysplasia (pre-malignant change in the epithelium with disordered growth and maturation) through to invasive carcinoma. This is known as the adenoma–carcinoma sequence . A typical colorectal adenocarcinoma is shown in Fig. 14.30a .

Our understanding of the processes involved in the development of cancer is critical in trying to prevent its occurrence. For example, simple public health interventions to promote improved dietary fibre intake have the potential to significantly reduce the risk of cancer development. Many developed countries have cancer screening programmes designed to prevent common cancers by detecting pre-cancerous changes and treating them before cancer develops, or to detect cancers in their earliest stages to allow effective curative treatment. Such systems are widely used to reduce the occurrence of cervical cancer and breast cancer. Screening for bowel cancer aims to identify patients with adenomas and early cancers. Such patients commonly have blood in their faeces and testing for this feature can be used to select those patients who will benefit from colonoscopy. If adenomas are identified, removal of these dramatically reduces the risk of future cancer development.
F follicle G malignant gland J anorectal junction LP lamina propria M mesoappendix MF mitotic figure Mu smooth muscle N necrosis RM rectal mucosa S serosa SM submucosa SS stratified squamous epithelium

Chronic inflammatory bowel disease includes two main conditions: ulcerative colitis and Crohn’s disease . These are relapsing and remitting inflammatory disorders with no known cause. Both conditions cause similar clinical and pathological findings so occasionally it may not be possible to distinguish between the two. Other differential diagnoses (see textbox ‘Disorders of the gastrointestinal tract’ ) also need to be considered as many other conditions are mimics of IBD.


Crohn’s disease (CD) can affect anywhere in the GI tract though it usually involves the small intestine. CD typically involves the GI tract in a patchy distribution with areas of normal bowel wall between affected areas (skip lesions). Inflammation is usually transmural, i.e. through the full thickness of the bowel wall, and associated with non-caseating granuloma formation .

Ulcerative colitis (UC) usually involves the rectum and can extend proximally to involve the colon. When active, inflammation is usually confined to the mucosa and submucosa. Granulomas are not a feature of UC. As UC is associated with repeated episodes of inflammation, ulceration and epithelial regeneration, this may lead to dysplastic change. This contributes to an increased risk of colorectal cancer in these patients.


Table 14.1 outlines the main structural features of the different components of the gastrointestinal tract for easy reference and revision. Please note that the epithelium of all segments includes stem cells and neuroendocrine cells, which have not been included in the table for simplicity. Each line of the table refers to the correspondingly labelled micrograph opposite.
| Part of the gastrointestinal tract | Type of epithelium | Main cell type of epithelium | Other distinctive features | Figure |
|---|---|---|---|---|
| Oesophagus | Stratified squamous | Squamous cells | Submucosal glands | 14.33a |
| Body/fundus of stomach | Glandular, straight tubular |
|
|
14.33b |
| Pylorus and cardia of stomach | Glandular, coiled, branched tubular |
|
|
14.33c |
| Duodenum | Glandular with villi and crypts of Lieberkühn |
|
|
14.33d |
| Jejunum and ileum | Glandular with villi and crypts of Lieberkühn |
|
|
14.33e |
| Colon and rectum | Glandular, straight crypts |
|
Taeniae coli | 14.33f |
| Appendix | Glandular, straight crypts |
|
Prominent lymphoid tissue | 14.33g |
| Anus | Stratified squamous | Squamous cells | Columns of Morgagni | 14.33h |









")





















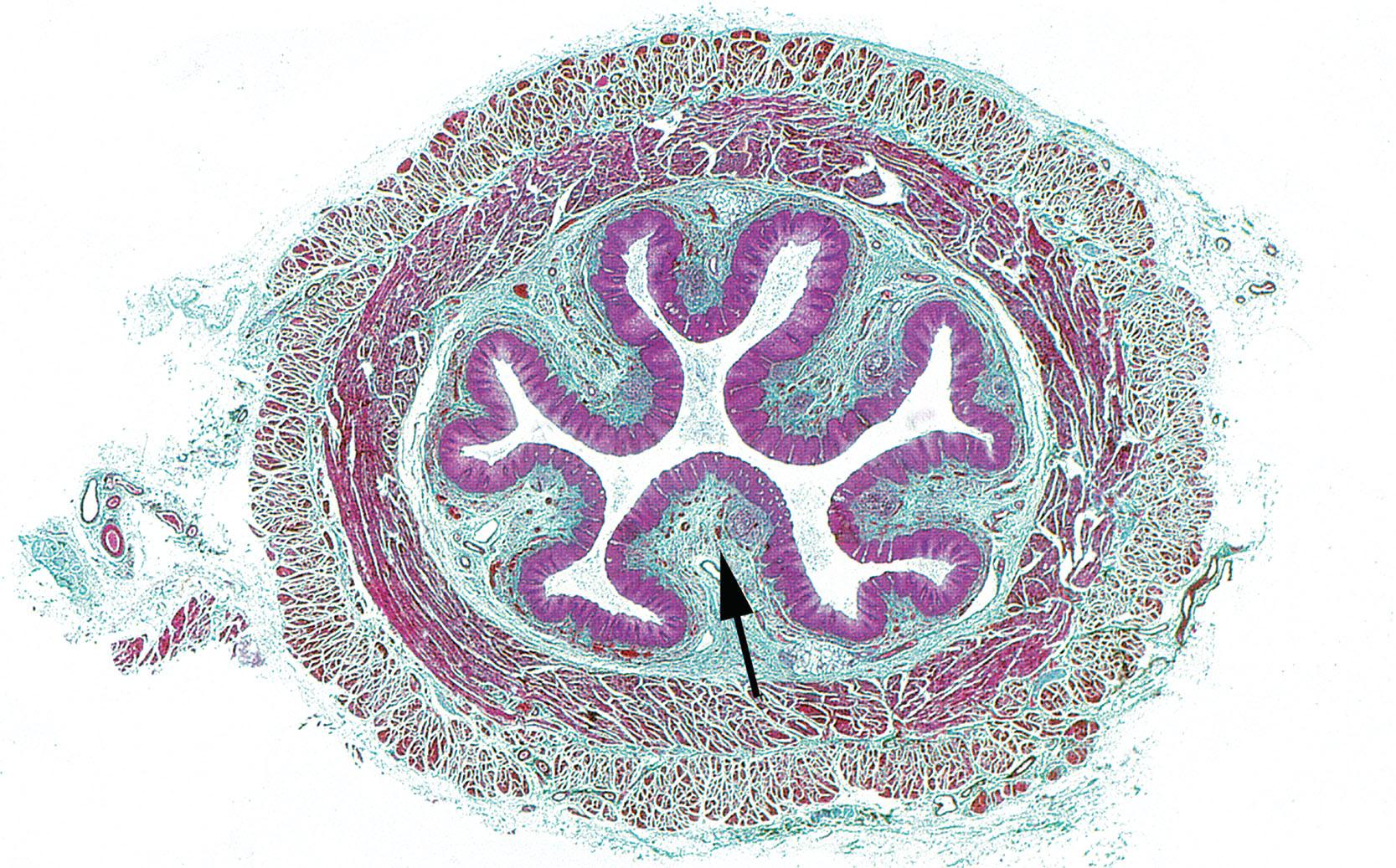
A whole section of oesophagus is illustrated in the image above. Which layer is highlighted by the arrow? (Select one answer):
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here