Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

A key requirement of being a good doctor is the ability to make a robust diagnosis. Making a diagnosis requires identifying departure from normal and involves answering two key questions:
Where is the problem (i.e. the anatomical site)?
What is the problem (i.e. nature of disease)?
A good history and a focused examination are the keys to making a diagnosis/differential diagnoses, and this is particularly true when patients present with diseases involving the gastrointestinal (GI) system. This chapter covers the key GI symptoms, how to take a focused history and the diseases likely to be associated with such symptoms. It then proceeds to cover examination technique for assessing the GI system, followed by a brief review of investigations required to confirm a diagnosis.
The human gastrointestinal tract can be seen as a system of serially connected tubular organs approximately 8 metres in length ( Fig. 14.1 ) including mouth, oesophagus, stomach, duodenum, jejunum, ileum, colon, rectum and anus which, together with its connected secretory glands including the salivary glands, pancreas and biliary tree within the liver, controls the passage, processing, absorption and elimination of food. Symptoms of gastrointestinal (GI) disorders usually arise owing to an alteration in this transit, or an alteration in the function of this system, which includes absorption, processing and elimination of food.
, includes all organs labelled in blue colour; hepatopancreaticobiliary (HPB), includes all organs labelled in orange colour; lower gastrointestinal (LGI), includes all organs labelled in green colour.")
The site of disease may lie in the lumen, its wall (including the mucosa, submucosa, muscle layer or serosa); involve the secretions that aid digestion (biliary and pancreatic diseases); and even lie outside the GI tract (extra luminal), affecting the GI system either through extrinsic compression or through neuroendocrine effects as seen in patients with diabetes or through electrolyte disturbances as in renal diseases. The liver, biliary system and pancreas, which are part of the GI system, are involved in aiding digestion. In addition, the liver is an important organ playing a key role in immunity as well as in metabolism of food and drugs, and also elimination of waste products such as bilirubin (a byproduct of haemoglobin breakdown) into bile.
Finally, from the standpoint of systematic history taking and examination, the kidneys, groin and genitalia are also considered in this chapter.
There are a large number of organs within GI tract, so to make it easier to diagnose the site of a problem, it may be helpful to consider the GI system composed broadly of three subsystems as follows:
Upper GI tract: This includes the oral cavity, oesophagus, stomach and proximal duodenum, traditionally as far as the ligament of Trietz: symptoms of diseases involving this section include dysphagia, odynophagia, reflux, heartburn, epigastric pain, and vomiting.
Lower GI tract: This includes small intestines, including distal duodenum, jejunum, ileum, colon, rectum and anus: common symptoms from diseases involving this section include change in bowel habit (this can range from constipation to diarrhoea, or a combination), bleeding per rectum, abdominal pain and distension.
Hepatopancreatico-biliary (HPB): This section includes liver, biliary tree including gall bladder and pancreas: diseases involving this section will present with symptoms that include jaundice and abdominal pain with biliary pain classically described as right upper quadrant abdominal pain radiating to the right shoulder. However, not all HPB diseases may be associated with jaundice and pure liver diseases rarely cause pain.
In addition to the above symptoms, GI diseases from all the three subsystems as above may present with diffuse or poorly localized abdominal pain, weight loss, loss of appetite and nausea. These symptoms, although of little localising value, may be useful in assessing the severity of underlying disease.
A wide variety of diseases are associated with different sites of the GI tract. For simplicity, one way of classifying these is based on the underlying causes as shown in Box 14.1 . However, in clinical medicine it is important to be aware of the common diseases and to include these in the differential diagnosis before considering rare ones. Table 14.1 includes list of common GI diseases.
V-Vascular: Ischaemic bowel, hepatic infarction
I-Inflammation/infection: Inflammatory bowel disease, viral hepatitis (A, B, C, D, E)
N-Neoplasms: Cancers of oesophagus, stomach, small bowel, colon, liver, pancreas, biliary tree
D-Drug (toxins)/degenerative/dysmotility: Drug-induced diarrhoea/hepatitis, irritable bowel syndrome
I-Iatrogenic/idiopathic: Perforation of GI tract post endoscopy, bleed post liver biopsy/trauma
C-Congenital/inherited/developmental: Pyloric stenosis, Hirschsprung’s disease
A-Autoimmune/allergy: Autoimmune hepatitis, coeliac disease
T-Trauma
E-Endocrine/metabolic/environmental: Diarrhoea caused by diabetic neuropathy
| Site | Diseases |
|---|---|
| Oesophagus | Oesophagitis, gastroesophageal reflux disease, hiatus hernia, oesophageal ulcer, benign oesophageal stricture, Barratt’s oesophagus, oesophageal cancer, oesophageal varices |
| Stomach | Gastritis, gastric ulcer, gastric cancer, gastric varices |
| Small bowel | Duodenitis, duodenal ulcer, coeliac disease, Crohn’s disease, lymphoma |
| Colorectal | Diverticulosis, ulcerative colitis, other colitis including infective, colonic/rectal polyps and cancers |
| Hepatic | Acute hepatitis, liver cirrhosis, liver abscess, liver cancers (primary/secondary) |
| Pancreatico-biliary | Gall bladder and CBD stones, cholangitis, cancer gall bladder and biliary tree, acute and chronic pancreatitis, cancer of the pancreas |
The common symptoms of GI and abdominal disease are listed in Box 14.2 and are discussed individually below.
Dysphagia and odynophagia
Heartburn and reflux
Indigestion
Flatulence
Vomiting
Anorexia
Constipation
Diarrhoea
Alteration of bowel pattern
Abdominal pain
Abdominal distension
Weight loss
Haematemesis
Rectal bleeding
Melaena
Jaundice
Itching
Urinary symptoms
An important aspect to remember while taking a history of GI symptoms is that certain symptoms and signs are associated with a higher likelihood of an underlying cancer, especially if recent in onset (i.e. less than 3 months in duration) and in an older patient (>55 years of age). These require urgent assessment, including referral to an appropriate specialist; to highlight this urgency such symptoms are referred to as red flags. The relevant red flags for GI diseases are shown in Box 14.3 .
Dysphagia
Dyspepsia: new onset lasting for weeks
Abdominal pain: new onset lasting for weeks
Change in bowel habit: diarrhoea or constipation, sense of incomplete evacuation
Rectal bleeding
Weight loss
Loss of appetite
New onset iron deficiency anaemia in non-menstruating women or in men
Dysphagia is defined as difficulty in swallowing. Patients may report an array of symptoms ranging from an awareness of something sticking in the throat or chest to an inability to swallow.
Dysphagia is a red flag symptom because it can be associated with oesophageal cancer or cancer of the gastric cardia or fundus. Other symptoms may accompany dysphagia and it is important to be familiar with the physiology of swallowing to understand the localizing value of these accompanying symptoms to help make an accurate diagnosis.
Swallowing is a complex movement composed of two phases: the initial oropharyngeal phase and the oesophageal phase ( Fig. 14.2 ). The oropharyngeal phase involves multiple actions that happen synchronously, which are designed to allow safe passage of food bolus from the mouth into the oesophagus, without it going into the trachea (aspiration) or refluxing in the nasal cavity. As the food is moved to the back of the mouth by the tongue, the tongue closes the oral cavity, the soft palate closes the nasal cavity and the epiglottis closes the larynx, so the food is safely propelled into the proximal oesophagus. Diseases affecting the oropharyngeal phase of swallowing include local diseases of the throat, such as cancer of the throat, which may present with symptoms of dysphagia. More commonly neurological conditions, such as stroke, affect swallowing and patients may present with symptoms of choking, recurrent aspirations with frequent chest infections and, rarely, reflux of food through the nose.

The second phase of swallowing is the oesophageal phase, initiated on entry of food bolus into the proximal oesophagus; it involves movement of food down the oesophagus by peristalsis aided by gravity and relaxation of the lower oesophageal sphincter (LOS) to allow passage of food into the stomach. Intact tone of the LOS is required to prevent reflux of gastric content into the oesophagus. Problems in the oesophageal phase can result in symptoms of dysphagia, reflux, heartburn and chest pain.
Box 14.4 shows the causes of dysphagia which can be broadly classified into obstructive and non-obstructive. Obstructive dysphagia may be caused by problems, firstly within the lumen such as foreign body, secondly within the wall, such as benign or malignant oesophageal strictures or thirdly extra-luminal compression of the lumen such as from goitre, thymoma, enlarged mediastinal lymph nodes or aortic aneurysm. Non-obstructive causes broadly refer to conditions that may affect oesophageal peristalsis, which can be caused by disorders within the oesophageal muscles—referred to as oesophageal dysmotility, the most prominent of these being localized to oesophagus such as achalasia of the cardia or eosinophilic oesophagitis or connective diseases such as systemic sclerosis. Dysmotility may also be owing to neurological disorders affecting the neuronal control of peristalsis, which include systemic diseases such as stroke, multiple sclerosis or myasthenia gravis.
Intraluminal: Foreign body
Within walls: Stricture, cancer
Extraluminal: Goitre, thymoma, mediastinal lymphadenopathy, compression from enlarged aorta or heart
Oesophageal: Achalasia cardia, eosinophilic oesophagitis, oesophageal dysmotility
Systemic: Stroke, multiple sclerosis, myasthenia gravis
Classifying dysphagia into obstructive and non-obstructive/dysmotility is relevant because these two types can be distinguished on the basis of an astute history, which should include questions in Box 14.5 .
Onset: Sudden versus gradual
Duration of symptoms: years or months or days
Is it worse with solids than liquids?
Difficulty in swallowing saliva
Accompanied with reflux
Loss of weight, loss of appetite, iron deficiency anaemia
The presence of dysphagia worse to solids would suggest an obstructive dysphagia; if it is progressively worse over a short time and accompanied with weight loss, then oesophageal malignancy should be suspected. A benign stricture (or rarely an oesophageal pouch) may follow the same pattern, but much less rapidly and only delayed weight loss. Neurogenic dysphagia may present with greater difficulty in swallowing with liquids than solids and, more importantly, may often be associated with aspiration or coughing and seen in patients with stroke, motor neuron disease and myotonic dystrophy.
In contrast, odynophagia is painful swallowing owing to inflammation in the oropharynx or proximal oesophagus, which may occur with or without dysphagia. Odynophagia indicates inflammation/infection of the oralpharyngeal or oesophageal mucosa, classically candida oesophagitis, which is commonly associated with recent therapy with steroids or antibiotics and the presence of diabetes. However, diffuse oesophageal candidiasis may be associated with immuno-compromised states, such as after chemotherapy or HIV infection.
Heartburn is a burning sensation perceived in the chest or neck. It is caused by acid reflux from the stomach into the oesophagus and seen in patients with gastro-oesophageal reflux disease (GORD). Occasionally it is difficult to distinguish from angina pectoris. It is reported as present particularly at night when the patient lies flat in bed or after bending or stooping when abdominal pressure is increased. Heartburn may be exacerbated by dietary intake (such as alcohol or very spicy or fatty foods, which lower tone of the lower oesophageal sphincter) and certain medications (such as bisphosphonates). However, not all patients with reflux will have symptoms of heartburn.
Reflux or regurgitation is a symptom which refers to non-acidic fluid or bile regurgitation into the mouth, causing a bitter taste and a disagreeable sensation retrosternally. It is suggestive of underlying GORD, but not all patients with GORD have reflux symptoms.
Dyspepsia, a medical term for indigestion, includes a wide variety of symptoms, such as epigastric pain, heartburn, distension, nausea or ‘an acid feeling’ occurring after eating or drinking, bloating and belching. It may be associated with diseases of the upper GI tract such as Helicobacter infection of stomach or duodenum, peptic ulcer disease and GORD. Upper GI malignancy should be excluded in older patients who present with a new onset of dyspepsia. It can also be associated with diseases of the biliary tree, such as chronic cholecystitis (inflammation of the gall bladder), or just the presence of gallstones.
Vomiting is forceful expulsion of gastric contents through the mouth or nose. It occurs either consequent upon an obstruction in the transit of food through the GI tract or as a neurogenic response, in turn triggered either by chemoreceptors in the brainstem or as a reflex from irritation of the stomach. Vomiting consists of a phase of nausea, followed by hypersalivation, pallor, sweating and hyperventilation. Retching, an involuntary effort to vomit, then occurs, followed by expulsion of gastric contents through the mouth and sometimes through the nose. Most nausea and vomiting of GI origin are associated with local discomfort in the abdomen. Non-GI disease, such as raised intracranial pressure or metabolic disturbance, should be suspected if vomiting is not associated with food or any preceding abdominal discomfort.
It is important to take a history of the content of the vomit, its relationship with meals, frequency and association with other symptoms such as abdominal pain or constipation. The content of the vomit varies with the nature of the food ingested and it is important to note the absence or presence of bile or blood. In pyloric stenosis, the vomit is usually copious and sour-smelling. It frequently contains recognizable food eaten many hours before and exhibits froth on the surface after standing, but no bile. Faeculent vomit, characteristic of advanced intestinal obstruction, is brown in colour, and has a faecal odour. Vomit containing formed faeces is rare and may indicate a fistula between stomach and transverse colon, usually from an invading colonic carcinoma.
Haematemesis, which is vomiting of blood, results from bleeding from lesions in the upper GI tract. Brisk haematemesis, such as from a large vessel in a gastric or duodenal ulcer, will cause the patient to vomit large volumes of pure blood. In addition this will often be accompanied with passage of black tarry stools, known as melaena (see below). Vomiting of dark-stained liquid is referred as coffee ground vomiting. It is owing to blood that lies in the acidic gastric juice for a period of time, during which it turns black and may be vomited looking like ground coffee. It is important to distinguish this from haemoptysis, which is coughing up blood and may be mixed with sputum.
Melaena, the passage of black, tarry stool, is often described as the 5s’: schwartz (black), sticky, smelly shiny, stool. The black colour is owing to blood as it gets denatured (digested), as it passes through the acidic milieu in stomach and long transit through the small bowel. It usually indicates bleeding in the upper GI tract. Less commonly, a small bowel bleed proximal to the ileo-caecal valve may produce melaena and, very occasionally, the bleeding source may be in the right colon, such as a large caecal polyp or cancer, with altered colour and partial digestion facilitated by slow transit.
Abdominal pain is one of the most common GI symptoms and can be produced by a wide variety of underlying diseases. As with any pain, it is important to characterize it in terms of its s ite, o nset, c haracter, areas of ra diation, t iming including duration and frequency, e xacerbating and relieving factors and associated features (the acronym SOCRATES is commonly used in practice as an aide-mémoire).
Acute abdominal pain is also discussed in Chapter 9 because it may be associated with serious life-threatening conditions and requires a distinct approach. The particular characteristics of pain from certain frequent and important causes are given in Box 14.6 . Abdominal pain often radiates or spreads from one site to another. The pattern of radiation can indicate specific diseases. Pancreatic pain classically radiates through to the back and is relieved on bending forward, whereas pain from passage of ureteric stone radiates from loin to groin on the respective side.
Peptic ulcer: Epigastric, burning or gnawing, radiates through to back, meal related, wakes the patient, relieved by antacid
Gastric cancer: Epigastric, severe, partly meal related, not relieved by antacid
Pancreatic: High epigastric, severe, felt front-to-back, immediately after eating, relieved by sitting forward
Midgut: Periumbilical, colicky, some relation to meals
Lower gut: Periumbilical or suprapubic, colicky, some relief from bowel action
Biliary: Right upper quadrant, severe, colicky (but over a long period of time), radiates to right shoulder, accompanied by nausea
Renal colic: Loin-to-groin, colicky, very severe, accompanied by nausea
Functional: Anywhere in the abdomen, colicky, accompanied by bloating, relieved by bowel action
It is important to be aware of referred pain in the abdomen when the pain is perceived away from the organ involved. The diaphragm is innervated by the phrenic nerve which derives from the C3,4,5 nerve roots. Hence, pain may arise from diaphragmatic irritation owing to an inflamed gall bladder in cholecystitis or a liver abscess abutting the right diaphragm may be referred to the right shoulder, whereas pain from splenic pathology may be referred to the left shoulder. Pain from renal diseases is often referred to the lumbar area anteriorly or posteriorly.
Abdominal pain may also be owing to causes that are not specifically in the abdomen such as metabolic disorders including diabetic ketoacidosis, porphyria or lead poisoning.
Abdominal distension is classically caused by one of the ‘Five Fs’: f luid (mainly ascites), f at (obesity), f oetus (pregnancy), f latus and f aeces. Consider whether the distension is symmetrical or asymmetrical. Common causes of symmetrical abdominal distension are obesity and ascites. Common causes of ascites include decompensated liver cirrhosis, congestive heart failure, nephrotic syndrome and abdominal malignancies.
Common causes of asymmetrical abdominal distension include marked enlargement of the major abdominal organs (hepatomegaly, splenomegaly) or the presence of a large mass lesion as seen in intra-abdominal cancers, lymphomas or peritoneal malignancies.
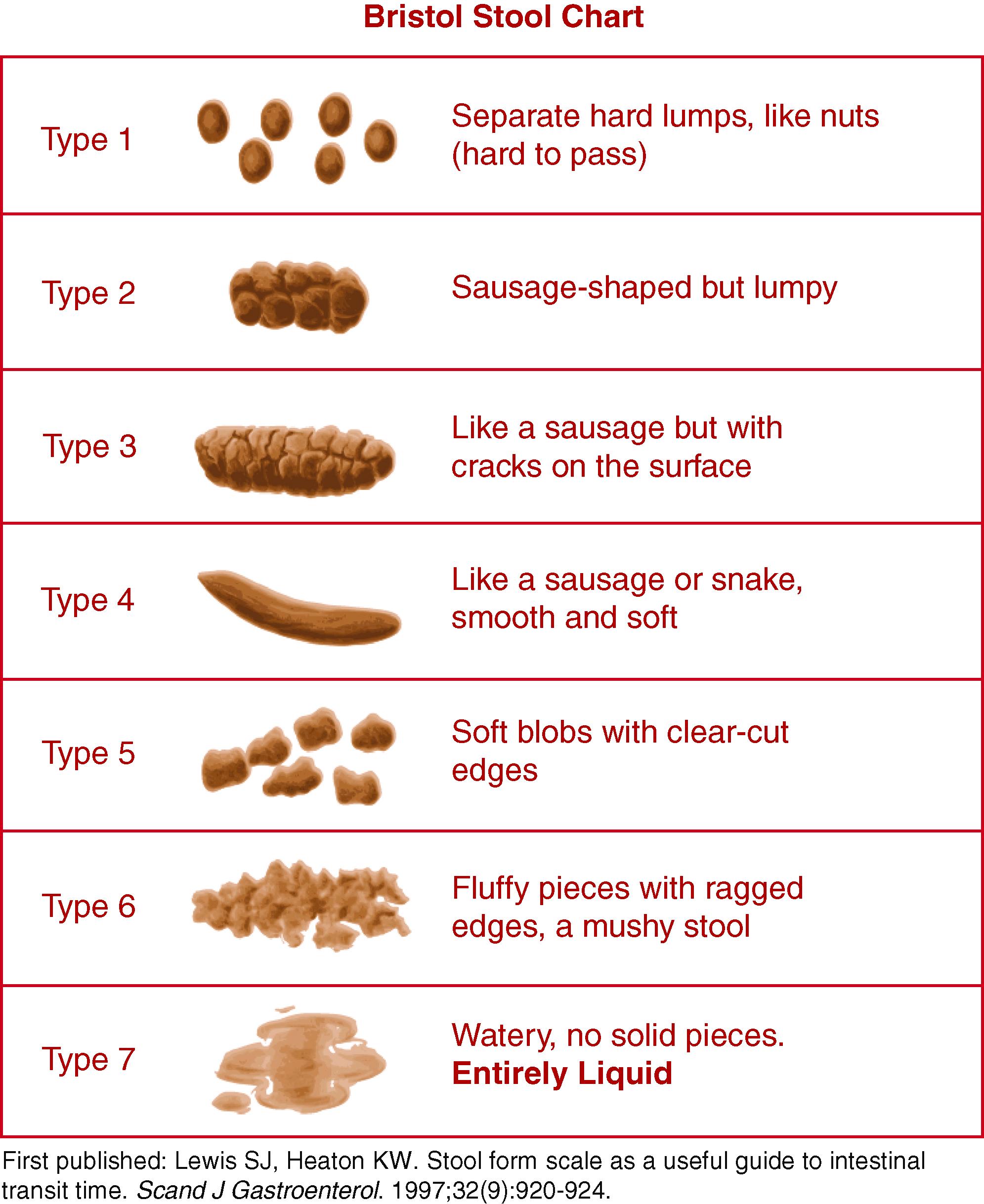
Change in bowel habit is a broad term that includes diarrhoea, constipation, as well as a combination, where patients may report alternating diarrhoea and constipation. The frequency of ‘normal’ bowel action varies greatly from person to person and within different parts of the world. In high-income countries, with a greater ingestion of processed food, the statistical norm varies between three bowel actions per day to three per week. It is important to use a Bristol Stool chart ( Box 14.7 ) to help objectively document the character of the stool, especially while monitoring response to an intervention or therapy.
Constipation refers to a reduction in the volume or frequency of stool and/or an increase in the hardness of stool. In clinical practice, the passage of formed stool less frequently than three times per week is usually taken to indicate an abnormality of bowel frequency. If unresponsive to simple treatment, such as increasing fibre in diet, drinking more water or simple laxatives, or if associated with red flag symptoms, then investigation may be needed. Common causes for constipation are shown in Table 14.2 and it may be useful to consider these while taking the history to assess constipation. Any new onset constipation that persists for weeks in a middle-aged patient is a red flag and requires urgent assessment, although is less concerning than an alteration to looser bowels.
| Types | Causes |
|---|---|
| Life style related | Low fibre, low fluid intake, drug related |
| Structural | Carcinoma, strictures, in colon or small bowel |
| Systemic | Metabolic (hypothyroid), neurological |
| Idiopathic/dysmotility | Irritable bowel syndrome |
Patients may report being constipated when they sense that they have not adequately emptied their bowel by defaecation, and this is referred to as sense of incomplete evacuation. It is important to identify this symptom because it may be associated with rectal lesions, including rectal cancers, and will require urgent assessment, especially if of recent onset. Tenesmus is pain in the peri-anal area during defaecation or the sense of needing to pass stool when there is none there.
Diarrhoea is an increase in the frequency of bowel movements; however, because there is a wide variation in the norm, it is important to establish in the history what was normal for a patient. However, passage of more than three stools per day or the passage of a large amount of stool (>300 g/day) will be considered as diarrhoea. It is important to ask the following key questions while taking a history of diarrhoea to help ascertain the likelihood of underlying diseases:
Is it acute (present for days/weeks) or chronic (greater than 3 months to years)?
Does it contain blood? Does it contain mucus?
Does it wake the patient in the night?
Is it accompanied by weight loss?
Acute diarrhoea commonly results from viral or bacterial infection, whereas longer periods of diarrhoea (chronic diarrhoea) may have a variety of causes as shown in Table 14.3 . The nature of the stool may give clues as to the underlying cause. In inflammatory bowel disease, the stool will be mixed with blood and mucus. The presence of blood in the stool excludes irritable bowel syndrome as the primary cause of any diarrhoea. In contrast, steatorrhoea is a distinct term that refers to the passage of pale, bulky stools containing excess fats that commonly float in water and are difficult to flush away. It is often described in patients with fat malabsorption owing to chronic pancreatitis with lipase deficiency or small bowel diseases with bile salt malabsorption. It is also important to distinguish diarrhoea from symptoms of incontinence or urgency as the underlying causes may be different.
| Causes | Clues | |
|---|---|---|
| Inflammatory | Infections, ulcerative colitis, Crohn’s disease | Blood in stools, abdominal pain, fever |
| Dysmotility | Irritable bowel syndrome | Abdominal pain Does not contain blood, not interrupt sleep |
| Malabsorption | Small bowel, pancreatic disease | Steatorrhoea, weight loss, anaemia |
| Secretory | Villous adenoma, ileal resection | Large volume No change with fasting |
Bleeding from the rectum or anal canal typically causes bright red blood loss that is separate from the stool or just noticeable on the toilet paper: haemorrhoids are the most common cause. If darker red and mixed with the stool, this usually indicates a source above the rectum, of which carcinoma is the most important cause. Haemoatochezia is passage of large-volume red blood per rectum and, if not from the colon, may indicate a potentially exsanguinating bleed from an upper GI source.
Flatulence describes passage of excessive wind. It is associated with belching, abdominal distension and passage of flatus per rectum. It is often associated with excessively swallowed air. In some patients it is associated with ingestion of certain foods, such as legumes, , broccoli and cabbage. It is a socially embarrassing symptom yet infrequently associated with structural diseases of the GI tract.
Jaundice (or icterus) is a yellowish pigmentation of the skin and conjunctival membranes caused by high levels of bilirubin in the blood, which is a waste product from the breakdown of red blood cells. Its presence implies disease of the liver or the biliary tract, although it may also be the result of excessive haemolysis. Jaundice may be classified depending on its cause as pre-hepatic, owing to excess bilirubin from haemolysis; hepatic, owing to diseases of the liver; or post-hepatic, caused by obstruction in the flow of the bile within the biliary tree owing to diseases of the biliary tree or pancreas. An important aspect of history taking is to be able to differentiate these three types of jaundice. The important questions to ask in the history are:
Presence of change in colour of urine
Presence of clay-coloured stools
Presence of itch
Haemolysis results in excess production of unconjugated bilirubin, which is water insoluble and does not get filtered in the urine. Hence, in jaundice caused by haemolysis, there is no change in colour of urine. In contrast, in hepatic and post-hepatic jaundice (also known as obstructive jaundice), the predominant type of bilirubin in the circulation is conjugated bilirubin which is water soluble and gets filtered out in the urine so the urine colour is darker or deeper yellow. In addition, post-hepatic jaundice is characterized by pale stools caused by a block in the passage of bile into the bowel and itch attributed to reflux of bile salts into the circulation. The differences between the three types of jaundice are shown in Table 14.4 . In addition to the characteristic colour of the skin and conjunctiva, there may be other associated cutaneous and systemic features of liver disease, often with dark urine (see below).
| Pre-hepatic | Hepatic | Post-hepatic | |
|---|---|---|---|
| History | No itch, Normal colour stools |
May have itch Normal/pale stools |
Itch Pale-coloured stool |
| Urine | Normal | Dark | Dark |
| Sclera | Lemon tinge | Dark | May fluctuate |
| Serum bilirubin | Often less than 70 | Variable | Can go very high Plateaus at 500 |
| Diseases | Gilbert’s, drug-induced haemolysis | Hepatitis, cirrhosis, liver cancer | Stones in common bile duct Cancer head of pancreas, biliary tree |
Pruritus or itch is a symptom associated with liver disease or obstructive jaundice. It is most often seen in patients with liver diseases, such as primary biliary cholangitis, primary sclerosing cholangitis and cholestasis of pregnancy where it may be the only symptom and not accompanied by jaundice. In contrast, it often accompanies jaundice in patients with carcinoma of the head of the pancreas or a cholangiocarcinoma. Pruritus is attributed to the presence of elevated bile salts and diminishes more quickly than the jaundice when the biliary obstruction is relieved.
Anorexia, which refers to loss of appetite, may be associated with a wide variety of conditions, both GI and non-GI-related. It is important to recognize the symptom of anorexia as distinct from the psychiatric illness anorexia nervosa . Another symptom to look for is early satiety where a patient may report feeling hungry but feels full after a few mouthfuls; this is indicative of decreased gastric capacity, either owing to extrinsic compression from an enlarged liver or spleen, an infiltrating type of gastric cancer called ‘linitis plastica’, which can reduce gastric capacity to distend, or more generally in patients with upper GI malignancy.
Weight loss may be owing to a decrease in food intake (as seen with anorexia, dysphagia or vomiting), malabsorption of nutrients or the effect of systemic diseases. Diseases that directly cause malabsorption include coeliac disease, pancreatic exocrine insufficiency and, occasionally, inflammatory bowel disease. Weight loss is also commonly associated with systemic conditions, such as cancer (within or outside the GI tract); chronic infections, such as tuberculosis (within or outside the GI tract); and endocrine conditions, such as thyrotoxicosis (despite an increased appetite) and Addison’s disease.
Urinary symptoms are discussed in Chapter 17 .
Physical examination involves a stepwise approach through the four steps of inspection, palpation, percussion and auscultation. In addition, for the GI tract, clusters of signs are linked with specific diseases and it is important to be aware of these as they provide clues to an underlying disease. Signs associated with chronic liver disease are shown in Box 14.8 ; of these, the most common and useful are spider naevi ( Fig. 14.3 ) (the presence of up to five can be normal) and palmar erythema ( Fig. 14.4 ) (the blotchy appearance often being more important than the overall redness). Inflammatory bowel disease may give rise to clubbing of the hands, arthritis, uveitis and skin changes, including erythema nodosum (tender raised red lumps on the extensor surface of the limbs) and the much rarer pyoderma gangrenosum. Anaemia accompanies many GI diseases, as does oedema, and lymphadenopathy can be secondary to GI malignancy.
Clubbing of the fingers
Leuconychia: Expansion of the paler half-moon at the base of the nail
Palmar erythema: Seen on the thenar and hypothenar eminence, often with blotchy appearance
Bruising
Dupuytren’s contracture: Can occur in the absence of liver disease
Hepatic flap: A sign of encephalopathy and advanced disease
Scratch marks: Particularly in cholestatic liver disease
Parotid swelling: Particularly in alcohol-related liver disease
Spider naevi: Small telangiectatic superficial blood vessels with a central feeding vessel
Hepatic foetor: Characteristic sweet-smelling breath
Gynaecomastia
Testicular atrophy: Loss of axillary and pubic hair
Pedal oedema

.")
It is helpful when examining the patient to record notes or communicate information to colleagues to remember the surface anatomy of the structures related to the GI tract and abdomen ( Figs 14.5 and 14.6 ) and to think of the abdomen as divided into regions ( Fig. 14.7 ). The two lateral vertical planes pass from the femoral artery below to cross the costal margin close to the tip of the ninth costal cartilage. The two horizontal planes, the subcostal and interiliac, pass across the abdomen to connect the lowest points on the costal margin and the tubercles of the iliac crests, respectively.



Wash your hands and introduce yourself (if you examining as a student on a ward round; if you took the history, you will have already introduced yourself).
Confirm the patient’s identity and explain the different steps of the abdominal examination in clear and easy to understand language, to seek patient agreement and consent for proceeding with the examination.
Position the patient appropriate for the examination: The patient should be lying supine with arms loosely at the sides, the head and neck supported by up to two pillows, sufficient for comfort. Make sure there is a good light, that the room is warm and that the hands are warm. A shivering patient cannot relax and vital signs, especially on palpation, may be missed.
Exposure of the abdomen: although it is important for the purpose of this examination that the area from ‘nipples to knees’ should be examined, it is not acceptable or appropriate to expose this area all at once. Instead, a stepwise approach is best, beginning with asking the patient to draw clothing up to just above the xiphisternum and a sheet folded down to the level of the symphysis pubis. The examination of the groins and genitalia must not be neglected and needs to be carried out with discretion, with full explanation as to the reasons, and leaving these areas exposed for a minimum amount of time. It is not unusual for a patient to present with intestinal obstruction owing to a strangulated femoral or inguinal hernia where the diagnosis has been missed initially owing to lack of proper inspection of the groins in an effort to save embarrassment.
The last thing before beginning the examination is to ask if the patient is in pain and if he is comfortable to proceed.
Inspection is an important and neglected part of abdominal examination. Initially, it is well worthwhile spending 30 seconds observing the abdomen from different positions to note the following features:
Is the abdomen of normal contour and fullness, or distended? Is it scaphoid (sunken)?
Generalized fullness or distension may be caused by fat, fluid, flatus, faeces or foetus.
Localized distension may be symmetrical and centred around the umbilicus as in the case of small bowel obstruction, or asymmetrical as in gross enlargement of the spleen, liver or ovary.
Make a mental note of the site of any such swelling or distension; think of the anatomical structures in that region and note if there is any movement of the swelling, either with, or independent of, respiration.
Remember that chronic urinary retention may cause palpable enlargement of the bladder felt in the lower abdomen.
A scaphoid abdomen is seen in advanced stages of starvation and malignant disease.
Normally the umbilicus is slightly retracted and inverted. If it is everted, then an umbilical hernia may be present; this can be confirmed by feeling an expansile impulse on palpation of the swelling when the patient coughs. The hernial sac may contain omentum, bowel or fluid. A common finding in the umbilicus of elderly obese people is a concentration of inspissated desquamated epithelium and other debris (omphalolith).
On inspection of the surface of the abdomen, look for the following characteristics: scars, striae, superficial veins, stomas and pigmentation.
Scars: Note any scars present, their site, whether they are old (white) or recent (red or pink), linear or stretched (and therefore likely to be weak and contain an incisional hernia). Common examples of post-surgery scars are given in Figure 14.8 .

Striae: Striae atrophica or gravidarum are white or pink wrinkled linear marks on the abdominal skin. Produced by gross stretching of the skin with rupture of the elastic fibres, they indicate a recent change in size of the abdomen, such as is found in pregnancy, ascites, wasting diseases and severe dieting. Wide purple striae are characteristic of Cushing’s syndrome.
Superficial veins: Look for prominent superficial veins, which may be apparent in three situations ( Fig. 14.9 : thin veins over the costal margin, usually of no significance; occlusion of the inferior vena cava; and venous anastomoses in portal hypertension). Obstruction of the inferior vena cava not only causes oedema of the limbs, buttocks and groins but, in time, distended veins on the abdominal wall and chest wall appear. These represent dilated anastomotic channels between the superficial epigastric and circumflex iliac veins below and the lateral thoracic veins above, conveying the diverted blood from the long saphenous vein to the axillary vein; the direction of flow is therefore upwards. If the veins are sufficiently prominent, try to detect the direction in which the blood is flowing by occluding a vein, emptying it by massage and then looking for the direction of refill. Distended veins around the umbilicus (caput medusae) are uncommon, but signify portal hypertension, other signs of which may include splenomegaly, ascites and other cutaneous manifestations of chronic liver disease. These distended veins represent the opening up of anastomoses between portal and systemic veins and occur in other sites, such as oesophageal and rectal varices.

Stomas: Stomas are surgically created openings in the abdominal wall and are identified by the presence of a stoma bag overlying these. There are three different types of stoma: a colostomy, an ileostomy or a urosotomy ( Fig. 14.10 ). The ileostomy, often on the right iliac fossa, is identified by an elevated spout. Colostomy stomas are often flat and can be either an end colostomy or a loop colostomy, in which case two lumens may be seen within the same stoma site. Urostomy is used to divert urine into a loop of bowel in the event of resection of urinary bladder.

Pigmentation: Pigmentation of the abdominal wall may be seen in the midline below the umbilicus, where it forms the linea nigra and is a sign of pregnancy. Erythema ab igne is a brown mottled pigmentation produced by constant application of heat, usually a hot water bottle or heat pad, on the skin of the abdominal wall or back. It is a sign that the patient is experiencing severe persistent pain, such as from chronic pancreatitis.
Palpation forms the most important part of the abdominal examination. Ask the patient to relax as much as possible, to breathe quietly and assure that you will be as gentle as possible. Enquire about the site of any pain and examine this region last. These points, together with unhurried palpation with a warm hand, will give the patient confidence and allow the maximum amount of information to be obtained.
When palpating, the wrist and forearm should be in the same horizontal plane where possible, even if this means bending down or kneeling by the patient’s side. The best palpation technique involves moulding the relaxed right hand to the abdominal wall, not to hold it rigid ( Fig. 14.11 ). The best movement is gentle but with firm pressure, with the fingers held almost straight but with slight flexion at the metacarpophalangeal joints and avoiding sudden poking with the fingertips ( Fig. 14.12 ).


Palpation of intra-abdominal structures is an imperfect process in which the great sensitivity of the sense of touch and pressure is heavily masked by the abdominal wall tissue. It is unusual for structures to be very easily palpable and so it is necessary to concentrate fully on the task and to try to visualize the normal anatomical structures and what might be palpable beneath the examining hand. It may be necessary to repeat the palpation more slowly and deeply. Putting the left hand on top of the right allows increased pressure to be exerted ( Fig. 14.13 ), such as with an obese or very muscular patient.

A small proportion of patients find it impossible to relax their abdominal muscles when being examined. In such cases, it may help to ask them to breathe deeply, to bend their knees up or to distract their attention in other ways. No matter how experienced the examiner, little will be gained from palpation of a poorly relaxed abdomen. It is important to keep in mind the following three signs on palpation which can be markers of serious intra-abdominal pathology.
Guarding is an involuntary reflex contraction of the muscles of the abdominal wall overlying an inflamed viscus and peritoneum, producing localized rigidity. It indicates localized peritonitis. What is felt on examination is spasm of the muscle, which prevents palpation of the underlying viscus. Guarding is seen classically in uncomplicated acute appendicitis. It is very important to distinguish this sign from the voluntary contraction of muscle.
Generalized or ‘board-like’ rigidity is an indication of diffuse peritonitis. It can be looked upon as an extension of guarding, with involuntary reflex rigidity of the muscles of the anterior abdominal wall. It is quite unmistakable on palpation; the whole abdominal wall feels hard and ‘board-like’, precluding palpation of any underlying viscus. The least downward pressure with a palpating hand in a patient with generalized rigidity produces severe pain. It may be differentiated from voluntary spasm by getting the patient to breathe: if there is voluntary spasm, the abdominal wall will be felt to relax during expiration.
Rebound tenderness is present if, when palpating slowly and deeply over a viscus and then suddenly releasing the palpating hand, the patient experiences sudden pain. Rebound tenderness is not always a reliable sign and should be interpreted with caution, particularly in those patients with a low pain threshold, but is often a useful adjunct to detecting peritoneal inflammation.
To ensure comprehensive assessment of all intra-abdominal structures, it is helpful to have a logical sequence to follow and, if this is done as a matter of routine, then no important point will be omitted. Always consider the underlying anatomy when examining the abdomen. The following scheme is suggested, which may need to be varied according to the site of any pain, palpating the site of pain towards the end:
Light palpation: Start in the left lower quadrant of the abdomen, palpating lightly, and move in an anti-clockwise direction including all nine areas of the abdomen; adopting this routine reduces the risk of missing signs.
Deep palpation: Repeat using slightly deeper palpation examining each of the nine areas of the abdomen.
Focused palpation:
Feel for the liver and gall bladder.
Feel for the spleen.
Feel for the left kidney.
Feel for the right kidney.
Feel for the urinary bladder.
Feel for the aorta and para-aortic glands and common femoral vessels.
Palpate both groins.
Examine the external genitalia.
If a swelling is palpable, spend time eliciting its features.
All of the organs in the upper abdomen (liver, spleen, kidneys, stomach, pancreas, gallbladder) move downwards with inspiration (with the spleen moving more downwards and medially). Thus, asking the patient to take a deep breath while examining makes detection of these organs easier. When the patient breathes in, the examining hand should be still so that the organ in question ‘comes on to the examining hand’ or ‘slips by underneath it’.
Place the right hand below and parallel to the right subcostal margin. The liver edge will then be felt against the radial border of the index finger ( Fig. 14.14 ). The liver is often palpable in normal patients without being enlarged. The lower edge of the liver can be clarified by percussion (see below), as can the upper border in order to determine overall size: a palpable liver edge can be owing to enlargement, or displacement downwards by lung pathology. Hepatomegaly conventionally is measured from the edge of the right costal margin in the mid-clavicular line. The degree of liver enlargement is often quoted in finger breadths, but these are variable and it is better to use centimeters. One helpful tip is to place the left hand over the right costal margin and use the right hand to assess for hepatomegaly, starting from the right iliac fossa and moving the right hand gradually upwards with each inspiration.

Try to discern the character of the liver surface (i.e. whether it is soft, smooth and tender as in heart failure, very firm and regular as in obstructive jaundice and cirrhosis, or hard, irregular, painless and sometimes nodular as in advanced secondary carcinoma). In tricuspid regurgitation, the liver may be felt to pulsate. Occasionally a congenital variant of the right lobe, called Riedel’s lobe, projects down lateral to the gallbladder as a tongue-shaped process. Although uncommon, it is important to be aware of this because it may be mistaken either for the gallbladder itself or for the right kidney.
The gallbladder is palpated in the same way as the liver, although the normal gallbladder usually is not palpable. When it is distended, however, it forms an important sign and may be palpated as a firm, smooth or globular swelling with distinct borders, just lateral to the edge of the rectus abdominis near the tip of the ninth costal cartilage. It moves with respiration. Its upper border merges with the lower border of the right lobe of the liver or disappears beneath the costal margin and therefore can never be felt ( Fig. 14.15 ). When the liver is enlarged or the gallbladder grossly distended, the latter may be felt not in the hypochondrium but in the right lumbar or even as low down as the right iliac region; hence, the importance of commencing palpation in the right iliac fossa and moving the examining hand upwards. An enlarged gallbladder may be easier to see moving on inspiration than to feel.

The ease of definition of the rounded borders of the gallbladder, its comparative mobility on respiration, the fact that it is not normally bimanually palpable and that it seems to lie just beneath the abdominal wall help to identify such a swelling as the gallbladder rather than as a palpable right kidney. A painless gallbladder usually can be palpated in the following clinical situations:
In a jaundiced patient with carcinoma of the head of the pancreas or other malignant causes of obstruction of the common bile duct (below the entry of the cystic duct), the ducts above the obstruction become dilated, as does the gallbladder (see Courvoisier’s law below).
In mucocele of the gallbladder, a gallstone becomes impacted in the neck of an uninfected gallbladder and mucus continues to be secreted into its lumen ( Fig. 14.16 ). Eventually, the uninfected gallbladder is so distended that it becomes palpable. In this case, the bile ducts are normal, and the patient is not jaundiced.

In carcinoma of the gallbladder, the gallbladder may be felt as a stony, hard, irregular swelling, unlike the firm, regular swelling in the two above-mentioned conditions.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here