Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

 and open (b).")
 ; with assisted ectropionized upper eyelid (b) .")
A conjunctivitis is an inflammation of the conjunctiva and causes red eye. It frequently occurs in individuals wearing contact lenses but can have multiple other causes, including viral or bacterial infections and allergies. Anemic patients display a whitish pale conjunctiva because of a low erythrocyte count. Eversion of the lower eyelid and inspection of the conjunctival sac is a simple diagnostic test for this condition.
[ G739 ]




a A stye (hordeolum) is a painful and frequently putrid inflammation of MEIBOMIAN glands on the inside of the eyelid or sebaceous glands at the outer rim of the eyelid (gland of ZEIS) usually caused by bacteria. A chalazion is usually the result of an occluded opening of the excretory duct of a MEIBOMIAN gland. Chalazia are painless.
b An inflammation of the rim of the eyelid can result in blepharitis with typical signs of a dry eye, including burning sensation. Blepharitis and generalized eyelid inflammation can cause hordeola and chalazia.
a [ G460, E964 ], b [ E282 ]







Topographical relationships of the orbit with neighboring regions (red).
Infections in these paraorbital regions can spread to the orbit and vice versa. Bony separations are often thin and pose no real barrier to the spread of aggressive germs.
[ L126 ]
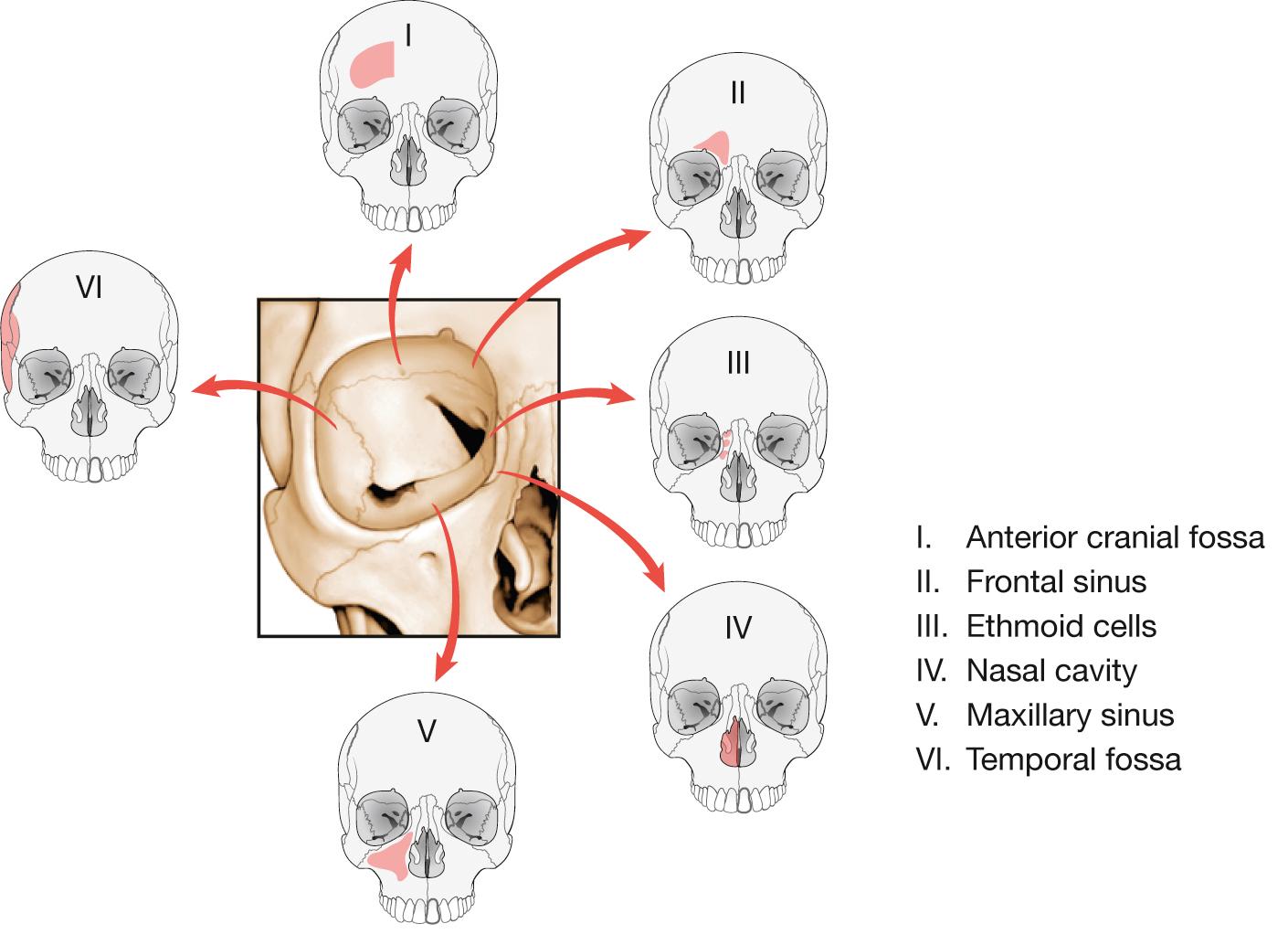
| Orbital Connections | Passageways |
|---|---|
| Anterior cranial fossa | Anterior ethmoid foramen |
| Middle cranial fossa | Superior orbital fissure and optic canal |
| Infratemporal fossa | Inferior orbital fissure |
| Pterygopalatine fossa | Inferior orbital fissure |
| Ethmoid cells | Posterior ethmoid foramen |
| Face | Infraorbital and zygomatico-orbital foramina |
| Nasal cavity | Nasolacrimal duct |
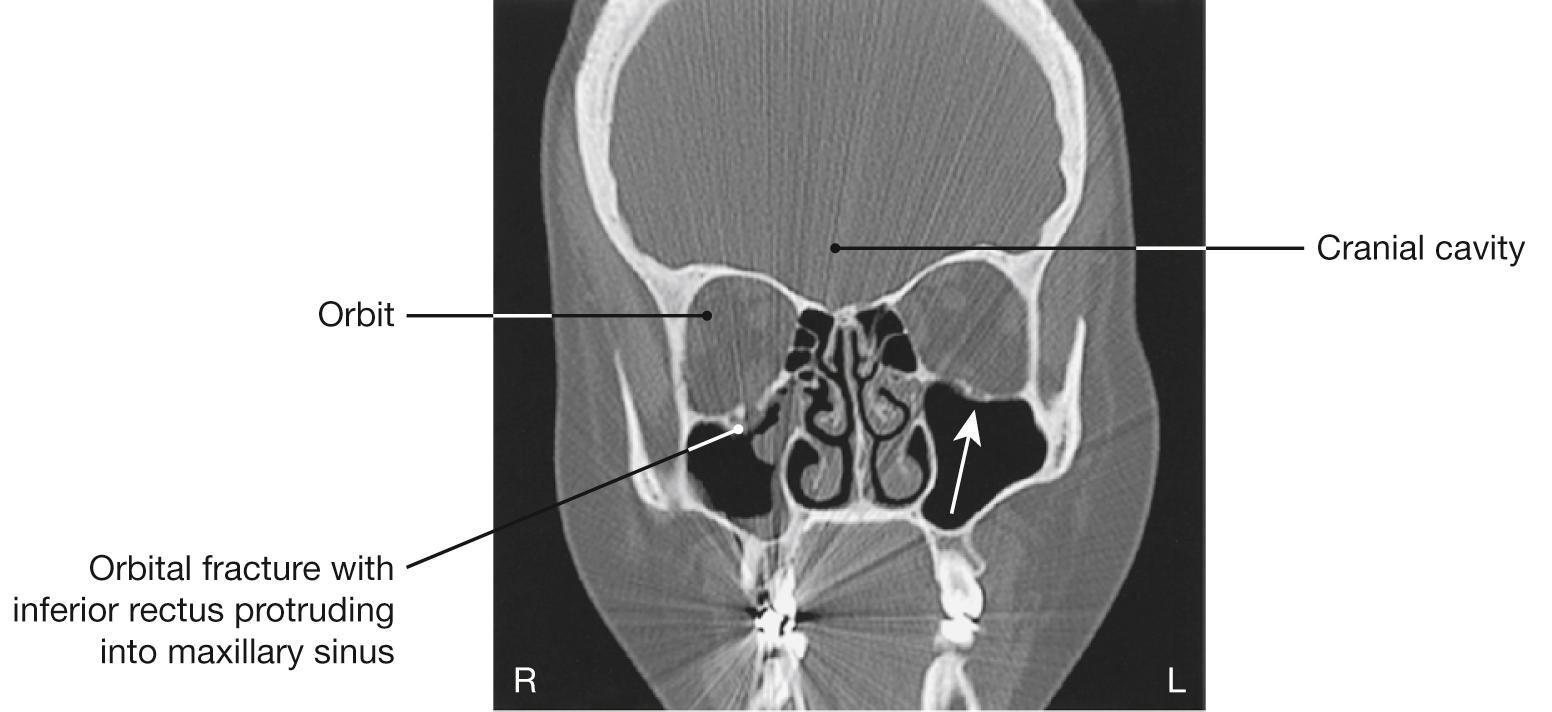
Blunt force to the eyeball (e.g. center blow to the orbit) can result in a fracture of the base of the orbit (blow-out fracture) as shown on the right eye in the CT image (arrow shows normal condition). As a result, infraorbital structures (inferior rectus and inferior oblique) can be trapped in the fracture gap or be forced into the maxillary sinus entirely (orbital hernia). Reduced mobility of the eye can cause double vision, enophthalmos, and/or the inability of this eye to look upwards. Involvement of the infraorbital nerve is likely if sensory dysfunction occurs in the dermal regions of the upper jaw because this nerve runs at the base of the orbit.
[ E402 ]



A retrobulbar hemorrhage can cause an acute retrobulbar compartment syndrome and is a medical emergency. The pressure in the orbit can cause ischemia to the optic nerve and retina resulting in blindness. To release the pressure, a lateral canthotomy is performed. The inferior crus of the lateral palpebral ligament (lateral canthal tendon) is cut to relieve the orbital compression. A lateral canthotomy is performed because the lateral aspect of the orbital entrance is devoid of major blood vessels and nerves ( Fig. 9.14 ).

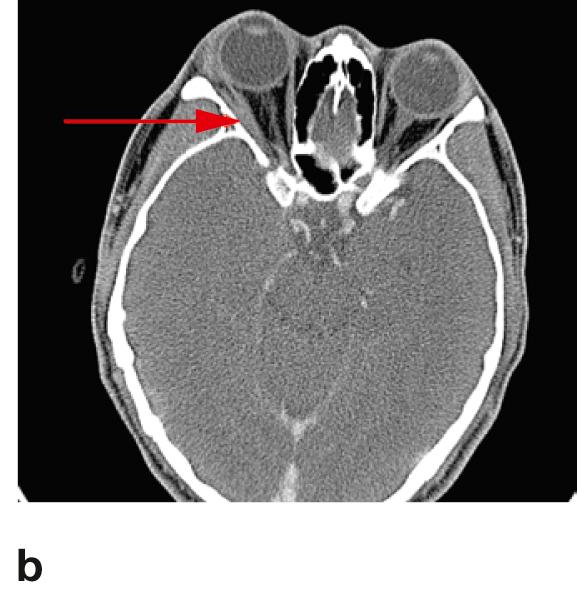
Right retrobulbar hemorrhage (a) with corresponding MRI (b); the red arrow indicates an extensive retrobulbar hemorrhage within the right orbit.

![Fig. 9.15, Arteries of the eye and of the orbit; superior view onto the opened orbit. [ E460 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Eye/21_3s20B9780702052736000090.jpg "Fig. 9.15, Arteries of the eye and of the orbit; superior view onto the opened orbit. [ E460 ]")

An ascending spread of germs from the facial region to the intracranial cavernous sinus occurs through drainage of venous blood via the facial vein, the angular vein in the nasal part of the orbit and the inferior ophthalmic vein. This can lead to an infection and thrombosis of the cavernous sinus . The first cranial nerve to be impaired is often the abducens nerve [CN VI] because of its central location within the sinus. Other cranial nerves affected are the oculomotor [CN III], trochlear [CN IV], ophthalmic [CN V/1] and maxillary [CN V/2] branches of the trigeminal nerve [CN V], resulting in paralysis of the extraocular muscles and facial sensory deficits.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here