Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The human nervous system consists of 30–40 billion nerve cells, which come into contact with each other via synapses. Functionally, the somatic (voluntary) nervous system is separated from the autonomic (involuntary) nervous system. The somatic nervous system controls all the processes which are subject to the human will and consciousness; the autonomic nervous system regulates the sympathetic, parasympathetic and enteric nervous system, in particular the activities and functions of the internal organs during physical exertion, digestion, resting, but also in emergency situations. Topographically, a distinction is made between the central nervous system (CNS) and the peripheral nervous system. The CNS consists of the spinal cord (Medulla spinalis) and the brain (encephalon). The latter has five subdivisions in a cranial to caudal order: cerebrum, diencephalon (‘intermediate’ brain), mesencephalon (midbrain), pons and Medulla oblongata or myelencephalon. The cerebellum, which together with the Medulla oblongata and pons forms the rhombencephalon, is located on the dorsal side of the pons. The brainstem includes the Medulla oblongata, pons and mesencephalon. With the exception of two cranial nerves, all nerves outside the spinal cord and the brain belong to the peripheral nervous system (PNS).
After working through this chapter, you should be able to:
explain the principles of the development of the nervous system;
name the internal structure of the cerebrum including the nuclei in sections/cuts of the brain;
name the meninges, relate them to the brain and spinal cord, as well as to the surrounding bony structures, and explain their innervation and blood supply;
explain the cerebrospinal fluid system in detail;
identify the large blood vessels supplying the brain, describe their segments and their pathways, and find and name their main bifurcations and terminal branches;
outline the Circulus arteriosus located at the cranial base and name its vessels;
place the functional cortical areas relatively to the supply areas of the cerebral arteries;
name the blood vessels of the Capsula interna;
explain the venous system of the Sinus durae matris, bridging veins and cerebral veins as well as venous anastomoses;
explain the fibre connections of the brain and their function;
describe the parts of the neocortex;
describe the areas of the hippocampus and explain how they connect to the ventricular system;
explain the individual parts of the Cortex cinguli as well as the areas of the paleocortex, and the olfactory cortical areas and functions;
explain the connections between the paleocortex and other areas of the brain, in particular the limbic system;
explain the arrangement, location and function of the central subcortical nuclei;
explain the components, organisational structure and functions of the diencephalon, thalamus, hypothalamus and epithalamus;
explain the parts of the brainstem and describe its functional systems, including important brainstem reflexes;
explain the surface, structure, blood supply, function and nuclei as well as the control and fibre systems of the cerebellum;
correctly name the twelve pairs of cranial nerves, their nuclei, exit points, pathways, and fibre qualities, the special position of the cranial nerves I and II, the respective target organs as well as their topographical position;
describe the segmentation of the spinal cord;
define the pyramidal and extrapyramidal system;
know the different neuronal functional systems;
describe the olfactory and gustatory system;
show a basic knowledge about different forms of pain;
describe the circuits of the visceral motor system, the structure of sympathetic and parasympathetic systems, including paravertebral and prevertebral ganglia, and show these on the dissection;
explain the enteric nervous system;
describe the visceral sensory system and its importance for autonomic reflex arches and control loops;
name parts of the autonomic nervous system, demonstrate the localisation of the centres, such as the respiratory centre and the cardiovascular centre, and describe the hypothalamus;
explain the limbic system, including its connections.
In order not to lose touch with prospective everyday clinical life with so many anatomical details, the following describes a typical case that shows why the content of this chapter is so important.
A successful 48-year-old project manager from the financial sector has hardly ever been to see a doctor. Because she has been suffering from headaches for several weeks, sometimes without any relief, she has gone to her GP. After a thorough medical history and physical examination, he prescribed strong painkillers and advised her to reduce her workload and to take up sport if possible. The painkillers improved the symptoms, but the headaches remained. She was able to go on holiday two months later and followed the doctor's advice to practice sport (jogging). Nevertheless, the headaches persisted. On a cycling tour with her husband she suddenly fell from the bicycle and lay twitching on the ground. Her husband sought medical help immediately, as she was unresponsive. When the ambulance arrived, the woman had become responsive, but was still very groggy. The ambulance took her to the nearest hospital, with her husband accompanying her.
When examined in the ambulance, the woman reported no other complaints besides the headaches and two painful grazes on the chin and right forearm. However, she was still slightly dizzy. During the initial examination in the hospital, the doctor on duty observes that the woman appeared to have urinated spontaneously. He asks her husband about details of the fall and previous illnesses. The husband describes his wife's ‘twitching’ after the fall, but says that she is otherwise always healthy. In the past few months she had frequently complained about severe headaches, supposedly because of her work load and had already been to the doctor, who had prescribed painkillers. After conducting a thorough physical examination to exclude fractures and internal injuries, the doctor arranges for a computed tomography of the head.
The CT shows a round, smoothly marginated mass with a strong and homogeneous uptake of contrast agent, making it look like a snowball ( Fig. a ). It is located at the cranial vault, in a parasagittal-right plane in the middle third of the Sinus sagittalis superior. Other pathologies or a trauma caused by the fall with the bicycle can now be ruled out. The CT finding and the seizure lead the radiologist to the suspected diagnosis of a meningioma.
Meningioma.
Due to the location, size and symptoms as well as the good general condition of the patient, she is advised to undergo immediate surgical removal of the tumour. She agrees and is transferred to the neurosurgery department, is given pre-operative information and is operated on the next day. After opening the cranium, the neurosurgeons can resect a confined, round, grey-white tumour of solid consistency, including the infiltrated dura mater, and thereby minimise the risk of relapse. For confirmation of the diagnosis, the resected tissue is brought to the pathology department.
The histopathologic examination with HE staining reveals grouped, uniform tumour cells, emerging from cells of the arachnoid mater and enveloped by collagenous septa.
 Many meningiomas contain small focal calcifications.
Many meningiomas contain small focal calcifications.
The result of the pathological-anatomical evaluation is a meningioma of the meningotheliomatous type, WHO grade I. This classification is especially important for the prognosis. Of all meningiomas, 90 % are of this type, i. e., they grow very slowly without infiltrating the brain and do not form metastases. The tumour is therefore classified as benign.
The dissection lab is the best place to get an idea of the location of the meninges. The three meninges (dura mater, arachnoid mater and pia mater) are very closely interlinked. Observing the meninges shows how and where a meningioma can develop from the cells of the arachnoid. As the arachnoid also surrounds the spinal cord, meningiomas are found throughout the cranial-spinal axis.
 Nine percent of patients have multiple meningiomas.
Nine percent of patients have multiple meningiomas.
Attention should be paid to the following intracranial predilection sites of meningiomas during dissection: the Falx cerebri, Sinus sagittalis superior, Alae ossis sphenoidalis, Tuberculum sellae, the olfactory groove and N. opticus.
Blood supply is guaranteed via meningeal branches of the A. carotis externa.
The indication for surgery depends on factors such as location, size, symptoms and the health status of the patient. Because they are mostly benign tumours with slow growth rates, very small meningiomas without clinical symptoms must often only be controlled. In the case of faster growth rates or incipient clinical symptoms as in the above-mentioned patient, a surgical procedure is indicated.
Further treatment options are fractionated or stereotactic radiation (radiotherapy), or the gamma knife.
The prognosis is particularly positive for grade I meningioma. Following complete removal of the tumour, the probability of relapse is approx. 9 % over the next five years. Long-term monitoring with MRI is often sufficient. The patient has already left the hospital and is now in a rehabilitation clinic. In eight weeks’ time, she can expect to return to her professional life.


If the rostral part of the neural tube does not close (open Neuroporus rostralis), the regular development of the three brain vesicles will not take place. Only a diffuse cluster of neural tissue is formed due to misdirected induction processes. The absence of brain development also results in an improper development of the skull. A facial skull is formed, but the brain and neurocranium are absent (anencephaly ). This developmental malformation is always fatal.








.")






The term encephalocele (hernia cerebri , cerebral hernia, outer brain prolapse, cranium bifidum) summarises defective developmental malformations with a median gap of the skull (at the root of the nose, or the forehead, cranial base, or occiput) ( Fig. a ). Protruding from this gap can be parts of the meninges ( meningocele , Fig. b ), or the brain ( meningoencephalocele , Fig. c ) without involvement of the cerebrospinal fluid spaces ( encephalocele, or d) including parts of the brain ventricles ( encephalocystocele, Fig. d , meningohydroencephalocele ).
![[ E347–09] [E347–09] [E347–09] [E347–09 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/17_3s20B9780702067679000125.jpg "[ E347–09] [E347–09] [E347–09] [E347–09 ]")
Head of a newborn with an extensive herniation in the occipital region. The upper red circle marks the defect in the area of the small fontanelle, the lower red circle indicates the defect in the area of the Foramen magnum.
The hernial sac of a meningocele is formed by the skin and meninges and is filled with cerebrospinal fluid.
The hernial sac of a meningoencephalocele contains parts of the cerebellum and is covered by the meninges and skin.
The hernial sac of this encephalocystocele is formed by parts of the Lobus occipitalis and part of the posterior horn of the lateral ventricle.

Spina bifida is a congenital cleft formation of the spine and the spinal cord caused by teratogenic substances (e. g. alcohol, medication) or the failed induction of the Chorda dorsalis.
In the case of a Spina bifida occulta ( Fig. a ) only the vertebral arches are affected. A vertebral cleft usually results from the failed fusion of one or two vertebrae. Hairy and strongly pigmented skin often covers the area of the defect. There are usually no clinical symptoms.
In the case of a Spina bifida cystica ( Fig. b ), the incomplete development of several adjacent vertebrae leaves a gap through which the meninges covering the spinal cord protrude cyst-like into the defect (meningocele). If the cyst also contains spinal cord and nerve tissue it is considered a meningomyelocele (usually associated with deficits).
A Spina bifida aperta (rhachischisis , myeloschisis , myelocele ; Fig. c ) is the most severe form of a cleft disorder of the vertebral arches and is combined with the inability of the neural folds to fuse. The undifferentiated neural plate is not covered by skin and lies fully exposed on the back. Newborns affected by such defects usually die shortly after birth. If the defect extends to the rostral end of the neural groove, the primordial brain does not develop (anencephaly).
![a, b [ E347-09], c [G617 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/19_3s20B9780702067679000125.jpg "a, b [ E347-09], c [G617 ]")






The clinical neurological examination includes a physical examination and the taking of a medical history to obtain information in particular on previous neurological diseases, cranial-cerebral trauma, congenital or familial neurological disorders, risk factors and autonomic functions. This is complemented by taking a symptom-focused history and specific diagnostic techniques to evaluate the cranial nerves and their corresponding functional systems. In addition, the physician should try a preliminary assessment of the patient's consciousness, orientation in space and time, memory function, concentration and basic mood. Disorders of the consciousness are clinically divided into somnolence (abnormal sleepiness but easy to wake up, delayed reaction to verbal communication, immediate response to pain stimuli), sopor (abnormally deep sleepiness and difficult to wake up, delayed but targeted defensive reaction to pain stimuli), and coma (cannot be woken up by external stimuli). A quantitative assessment of impaired states of consciousness, e. g. within the context of a follow-up, can be attained with the Glasgow coma scale . The severity of a consciousness disorder is quantitatively evaluated by testing the patient's spontaneous activity, and his or her response to verbal requests and pain stimuli, and scoring these reactions with points. Disorientation, confusion and perception disorders (e. g. in the context of an alcoholic or drug delirium) can lead to substantial disturbance of consciousness.







Atrophy of the brain develops with advanced age. This is associated with a widening of the sulci and a narrowing of the gyri. However, the decreasing memory function which accompanies advanced age is not directly linked to this atrophy of the brain, but is caused above all by a shorter duration of the deep sleep phases. With ageing, the proportion of deep sleep will diminish significantly. Up to the 26 th year of life, 19 % of total sleep duration is spent in deep sleep phases. Between 36 and 50 years of life this percentage drops to 3 %. Studies have shown that this correlates to significant decreases in memory function.
.")


.")








| Fibre system | Connection |
|---|---|
| Association fibres | |
| Fasciculus longitudinalis superior | Lobus frontalis with Lobus parietalis and Lobus occipitalis |
| Fasciculus longitudinalis inferior | Lobus occipitalis with Lobus temporalis |
| Fasciculus arcuatus | Lobus frontalis with Lobus temporalis (BROCA's area with WERNICKE's area) |
| Fasciculus uncinatus | Lobus frontalis with basal Lobus temporalis |
| Cingulum | lower parts of the Lobus frontalis with lower parts of the Lobus parietalis and Lobus parahippocampalis |
| Commissural fibres | |
| Corpus callosum | Frontal, parietal and occipital lobes of both hemispheres |
| Commissura anterior | Tractus olfactorius; anterior parts of the Lobus temporalis (amygdala; Gyrus parahippocampalis) of both hemispheres |
| Commissura posterior | Nuclei commissurae posteriores of both hemispheres |
| Commissura fornicis | Hippocampus of both hemispheres |
| Projection fibres | |
| Tractus corticospinalis | Cortex (especially Gyrus precentralis) with spinal cord |
| Tractus corticopontinus | Cortex with nuclei of the pons (Nuclei pontis) |
| Tractus corticonuclearis | Cortex with nuclei of the cranial nerves in the mesencephalon, pons and Medulla oblongata |
| Fornix | Hippocampus with parts of the limbic system and the diencephalon |
| Fasciculi thalamocorticales | Thalamus with cortex |
The developmental failure of the primordial structure (agenesis) of the Corpus callosum is, with three to seven cases per 1,000 births, a relatively common malformation in humans. It can have a wide range of causes and may be associated with absent or underdeveloped connections between the left and right hemispheres, without inevitably leading to changes in behaviour. The clinical signs and symptoms depend largely on the cause. It often presents with neuropsychiatric deficits and difficulties in problem-solving behaviour, in the understanding of language and grammar, or in the verbal description of emotions (alexithymia).
Although the neurosurgical resection of the Corpus callosum (callosotomy ) is a treatment option in patients with therapy-resistant epilepsy, it is only practised in exceptional cases. In patients who have undergone this treatment (split-brain patients ) , the information processed in the right half of the brain can no longer be transmitted to the left dominant hemisphere and thereby to the cortical language centres. They can recognise and also describe such information, but are not able to name it precisely.


If a cerebrocranial trauma is accompanied by rupture of the dura mater and the arachnoid mater, e. g. in the area of the nose or ear, this can lead to a fistula of cerebrospinal fluid (CSF fistula ) . This means that cerebrospinal fluid runs out of the nose (rhinoliquorrhoea) or out of the ear (otoliquorrhoea ). To test for the presence of a CSF fistula, a small amount of the fluid is collected to determine its content of glycoprotein β 2 -transferrin, as this isoform only occurs in the CSF.
Epidural anaesthesia (epidural) is a standard anaesthetic method. After the insertion of a cannula into the epidural space (without penetrating the dura), local anaesthetics can be injected. These anaesthetics act on the spinal roots and spinal ganglia. The epidural is used for the regional elimination of pain, for example in obstetrics, when surgical procedures cannot or do not need to be conducted under general anaesthesia.











 from the inner to the outer subarachnoid spaces.")


Meningiomas are slow-growing, usually benign intracranial tumours. They develop predominantly in the area of the PACCHIONIAN granulations (Granulationes arachnoideae), along the Falx cerebri, in the area of the sphenoidal wings, and in the olfactory groove. They mostly originate from mesothelial cells in the arachnoid mater. Initially, they often remain unnoticed because the surrounding tissue can adapt to the tumour growth rate. So they can achieve a significant size before causing symptoms, e. g. a sudden seizure or increasing headaches. If a surgical resection is possible, the prognosis is very good.
In contrast to the brain and spinal cord, the meninges are extremely well innervated and therefore very pain-sensitive. This is particularly apparent in patients with meningitis, who suffer from severe headaches, accompanied by stiffness of the neck and overextension of the spine (meningismus ). A suspected meningismus can be diagnosed with two tests:
(1) If the head of a supine patient is passively bent forward, and this leads to a reflexive flexion of the legs for pain relief (decompression of the meninges), the BRUDZINSKI's sign is positive.
(2) For a positive KERNIG's sign , the passive lifting of the straightened leg triggers an active flexion of the knee joint due to irritation of the meninges.

| Ventricle, section | Wall | Adjacent structures | Plexus choroideus |
|---|---|---|---|
| Ventriculi laterales, Cornu frontale | Roof | Corpus callosum (truncus) | No |
| Anterior wall | Corpus callosum (genu) | ||
| Medial wall | Septum pellucidum | ||
| Lateral wall | Caput nuclei caudati | ||
| Ventriculi laterales, Pars centralis | Roof | Corpus callosum | Yes |
| Floor | Thalamus | ||
| Medial wall | Septum pellucidum, Fornix | ||
| Lateral wall | Corpus nuclei caudati | ||
| Ventriculi laterales, Cornu occipitale | Roof | Medullary body of the Lobus occipitalis | No |
| Floor | Medullary body of the Lobus occipitalis | ||
| Medial wall | Calcar avis | ||
| Lateral wall | Radiatio optica | ||
| Ventriculi laterales, Cornu temporale | Roof | Cauda nuclei caudati | Yes |
| Floor | Hippocampus | ||
| Medial wall | Fimbria hippocampi | ||
| Lateral wall | Cauda nuclei caudati | ||
| Anterior wall | Amygdala | ||
| Ventriculus tertius | Roof | Tela choroidea ventriculi tertii | Yes |
| Floor | Hypothalamus | ||
| Anterior wall | Lamina terminalis ventriculi tertii | ||
| Lateral wall | Thalamus, epithalamus | ||
| Ventriculus quartus | Roof | Velum medullare superius cerebelli and Velum medullare inferius cerebelli | Yes |
| Floor | Fossa rhomboidea | ||
| Lateral wall | Pedunculi cerebelli |
 of the fornix.")





| Ventricle | Artery |
|---|---|
| Ventriculi laterales |
|
| Ventriculus tertius | A. choroidea posterior medialis (from the A. cerebri posterior) |
| Ventriculus quartus |
|

Due to their blood-CSF barrier instead of a blood-brain barrier, the circumventricular organs serve as pharmacological access routes. In the case of fever, for example, acetylsalicylic acid (ASA) has an antipyretic action as inhibitor of cyclooxygenase by reducing the production of prostaglandin. In the case of fever, the temperature-sensitive neurons of the Organum vasculosum laminae terminalis have a reduced sensitivity for intrinsic prostaglandins. These neurons normally initiate cooling mechanisms, which in the case of fever only function to a minor extent or not at all. By reducing the prostaglandin formation, ASA can therefore increase the sensitivity of neurons. As a result, the downregulation of the set-point caused by the fever is readjusted to the standard value – and the high temperature/fever is lowered. Central vomiting (emesis), e. g. due to opioids, can be treated with neuroleptic drugs, which bind to dopamine receptors in the Area postrema and thus have an antiemetic effect.
Obstructions of CSF drainage ( Fig. a CT scan image) can be caused by tumours, malformations, bleeding or other factors, and due to increased intracranial pressure they can lead to headaches, nausea and a papilloedema ( Fig. c image of ocular fundus). In the case of a blockage in the inner CSF space, a hydrocephalus internus will occur and impaired drainage in the outer CSF or subarachnoid space will lead to a hydrocephalus externus . Hydrocephalus e vacuo is the term for a condition when ventricular size considerably increases because of a loss of brain substance, e. g. as in ALZHEIMER's disease.
The circumventricular organs ( Fig. 12.47 ) lack the blood-brain barrier and are thus capable of monitoring the plasma-blood milieu; as such they are of more interest than at a purely pharmacological level. The Area postrema for example contains numerous dopamine and serotonin receptors. Highly promising anti-emetic effects can be achieved by using dopamine or serotonin antagonists. In addition, the excitability of biochemical receptors in the Area postrema is a protective mechanism for the whole body, for example by centrally triggered vomiting after the ingestion of spoiled food, so that the major part of the potentially harmful substance is eliminated from the body.
![[ R317 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/69_3s20B9780702067679000125.jpg "[ R317 ]")
Computed tomographic (CT) cross-section of the head of a female patient with impaired CSF drainage ( Fig. a ) due to a narrowing of the Aqueductus mesencephali [aqueduct of SYLVIUS] . The ventricles are significantly enlarged at the expense of the parenchyma of the brain (hydrocephalus ). The patient suffered from massive intellectual deficits and significant gait disorders. For comparison, a CT scan of a healthy person is shown ( Fig. b ).
![[ S700 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/70_3s20B9780702067679000125.jpg "[ S700 ]")
Ocular fundus, Fundus oculi; left side; anterior view; ophthalmoscopic image of the central area showing a congested Papilla nervi optici due to increased cranial pressure. A congested Papilla nervi optici (optic disc) is visible on the ocular fundus as a clinical sign of an intraventricular neurocytoma WHO grade II. As the N. opticus [II] is surrounded by meninges and fluid, the optic disc bulges in the eyeball.

The cerebral blood flow has great clinical relevance. Lack of oxygen will irreversibly damage brain tissue (ischaemia tolerance ) within a maximum time of 7–10 min. This must be taken into account in the cardiovascular resuscitation of patients in cardiac arrest. The importance of brain circulation is immediately clear when standing up too quickly leads to a blackout, because the brain is momentarily not sufficiently supplied with blood. The same occurs with fainting (syncope ). The brain is not supplied with enough blood, and as a result, the patient drops to the floor. When lying down, the cerebral blood flow improves and the brain functions return.
Vascular changes (extracranial arteriosclerosis: plaques, stenosis, obliteration) are often located in the carotid bifurcation . The Glomus caroticum (not shown in Fig. 12.48 , Fig. 12.158 ) is a paraganglion located in the carotid bifurcation; it contains chemoreceptors, which react to changes of the pH, oxygen and carbon dioxide levels of the blood.
The carotid sinus syndrome is defined as a hypersensitivity of pressure receptors in the carotid sinus and may often be triggered in response to a rotation of the head. This initiates a reflex that strongly lowers the heart rate (vasovagal reflex ) which can result in cardiovascular collapse and cardiac arrest.


| Artery | Segment | Topography/anatomical structures |
|---|---|---|
| A. carotis interna, ICA = internal carotid artery | C1 – cervical | Pars cervicalis |
| C2 – petrous | Pars petrosa up to the end of the Canalis caroticus | |
| C3 – lacerum | up to a ligament between Lingula sphenoidalis and the apex of the Os petrosum (‘Lig. petrolingualis’) | |
| C4 – cavernous | in the Sinus cavernosus until exiting the dura below the Proc. clinoideus | |
| C5 – clinoid | between Proc. clinoideus anterior and the base of the Os sphenoidale | |
| C6 – ophthalmic | up to the outlet of the A. communicans posterior; outlet of the A. ophthalmica | |
| C7 – communicating | up to the bifurcation of the ICA into the Aa. cerebri anterior et media | |
| A. cerebri anterior, ACA = anterior cerebral artery | A1 | Pars precommunicalis; from its origin to the outlet of the A. communicans anterior |
| A2 | Pars postcommunicalis; from the outlet of the A. communicans anterior to the outlet of the A. callosomarginalis; also: Pars infracallosa | |
| A3 | Pars postcommunicalis; distally of the outlet of the A. callosomarginalis (A. pericallosa); some authors differentiate even more segments (A4 and A5) | |
| A. cerebri media, MCA = middle cerebral artery | M1 | Pars sphenoidalis; from its outlet to the bifurcation in two or three main branches |
| M2 | Pars insularis; in the Fossa lateralis, above the insula | |
| M3 | Pars opercularis; in the Fossa lateralis, lateral branches in the direction of the cortical surface | |
| M4 | Pars terminalis; after the exit of all vessels from the Sulcus lateralis | |
| A. cerebri posterior, PCA = posterior cerebral artery | P1 | Pars precommunicalis; from its outlet to the A. communicans posterior; passes through the Cisterna interpeduncularis |
| P2 | Pars ambiens; from the A. communicans posterior to the outlet of the Rr. temporales anteriores (at the level of the Cisterna ambiens) | |
| P3 | Pars quadrigeminalis; from the Rr. temporales anteriores to the bifurcation into the Aa. occipitales medialis and lateralis (at the level of the Cisterna quadrigeminalis) | |
| P4 | Pars calcarina; terminal branches: A. occipitalis medialis and A. occipitalis lateralis | |
| A. vertebralis, VA = vertebral artery | V1 | Pars prevertebralis |
| V2 | Pars transversaria | |
| V3 | Pars atlantica | |
| V4 | Pars intracranialis |




Arteriosclerotic changes in vascular walls are relatively common findings at the outlet of the A. carotis interna from the A. carotis communis, as well as in the Pars cavernosa.
More than 90 % of all cerebral aneurysms occur in the basal cerebral vessels of the Circulus arteriosus cerebri [WILLIS] (figure). Most often, the A. communicans anterior (ACA, up to 40 %) and the A. carotis interna are affected. During the surgical removal of an aneurysm in the A. communicans anterior, care must be taken not to sever the A. centralis longa (syn.: A. striata medialis distalis, A. striata longa , A. recurrens, HEUBNER's artery ). This artery is a branch which mostly originates laterally descending from the proximal A2 segment or the distal A1 segment of the A. cerebri anterior ( Fig. 12.63 ) and runs anti-parallel back to the initial segment of the A. cerebri anterior. In addition, care should be taken to avoid the other branches of the A. communicans anterior, as otherwise postoperative disorders of the memory function could occur (syndrome of the A. communicans anterior ).
![[ G749 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/78_3s20B9780702067679000125.jpg "[ G749 ]")
Normally, ( Fig. a ) blood flows cranially from the aortic arch (caudal) through both arterial systems supplying the brain (black arrows) to reach the circle of WILLIS, Circulus arteriosus cerebri [WILLIS]. A patient with subclavian steal syndrome (b) frequently has a proximal high grade stenosis of the left A. subclavia. Intense physical activity with the left arm results in retrograde (reverse) blood flow in the left A. vertebralis (affected side, red arrows, Fig. b ). This causes the brain to receive less blood (thin arrows, Fig. b ) which may mean dizziness and headaches. The A. subclavia sinistra is usually affected in patients with subclavian steal syndrome.
![[ S701-L126 ]](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/79_3s20B9780702067679000125.jpg "[ S701-L126 ]")



![Fig. 12.56, Arterial circle of the brain, circle of WILLIS, Circulus arteriosus cerebri [WILLIS]; superior view.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/84_3s20B9780702067679000125.jpg "Fig. 12.56, Arterial circle of the brain, circle of WILLIS, Circulus arteriosus cerebri [WILLIS]; superior view.")
Most cerebral aneurysms are congenital defects of the Tunica media in the vascular wall at the points where it branches out. Often, aneurysms are associated with other diseases, such as polycystic kidneys or fibromuscular dysplasia. Cerebral aneurysms are usually asymptomatic. However, the pressure of the aneurysmal sac can lead to a cranial nerve compression.
Cerebral aneurysms have a tendency to rupture and are the most frequent cause of subarachnoid bleeding (haemorrhage). In the case of a rupture, sudden severe headaches occur, combined with vomiting and impaired consciousness.
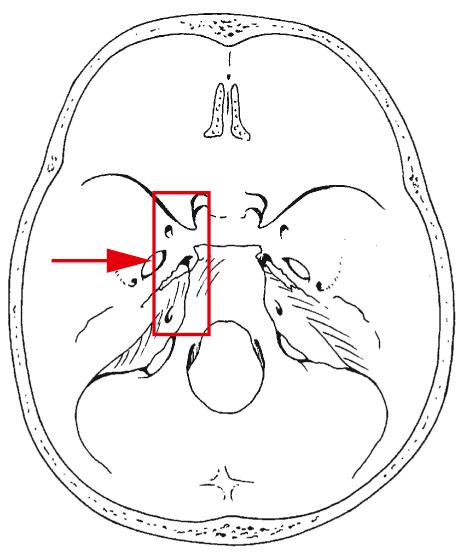
![Fig. 12.57, Passageways of vessels and nerves through the internal surface of the cranial base, Basis cranii interna, and arterial circle of the brain, Circulus arteriosus cerebri [WILLIS]; superior view.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Brainandspinalcord/85_3s20B9780702067679000125.jpg "Fig. 12.57, Passageways of vessels and nerves through the internal surface of the cranial base, Basis cranii interna, and arterial circle of the brain, Circulus arteriosus cerebri [WILLIS]; superior view.")

The blood vessels supplying the brain show relatively great variations in their pattern, which correspond to the variability of the supplied areas. Disorders of the blood flow in these ‘atypical’ vessels can therefore lead to stroke symptoms that cannot be explained in terms of the normal ‘textbook’ anatomy. Not without reason do we say: ‘The exception proves the rule.’

One of the most frequent types of cerebral circulatory disorders (ischaemia) in the vertebral arterial system is the so-called WALLENBERG's syndrome (dorsal-lateral Medulla oblongata syndrome ). In this case, an occlusion or impaired blood flow in the A. inferior posterior cerebell i (PICA = posterior inferior cerebellar artery ) causes a broad range of symptoms, including nystagmus, vestibular disorder, dizziness (Nuclei vestibulares, inferior olive), ipsilateral hemiataxia (Pedunculus cerebellaris inferior, cerebellum), contralateral dissociated sensations (Nuclei gracilis et cuneatus, Tractus spinothalamicus), swallowing difficulties, an attack of hiccups (singultus) and dysphonia (Nucleus ambiguus), HORNER's syndrome and a rapid pulse (central sympathetic system and cardiovascular centre in the rostral-ventrolateral Medulla oblongata), as well as respiratory disorders (respiratory centre in the ventrolateral Medulla oblongata with pre-BÖTZINGER complex).

In most cases a stroke is caused by an acute circulation disorder in a smaller or larger brain area supplied by the affected cerebral artery (ischaemia, brainstem infarction (BSI), 80–90 % of cases). Acute bleeding in the brain (intracerebral haemorrhage) accounts for nearly 10 % of all strokes, followed by subarachnoid haemorrhages (approx. 3 %). The first diagnostic measure to confirm or exclude a haemorrhage, ischaemia or a totally different cause of the neurological symptoms, is a CT of the brain. The speed of the CT-imaging makes it the preferred choice over MRI-imaging. With modern equipment, CT scans of the brain can now be obtained in less than half a minute. If the ischaemia is caused by a thrombus, a pharmacological therapy (thrombolysis) can be attempted. The outcome is largely determined by how much time has lapsed since the stroke (‘time is brain’). Many clinical centres therefore have specialised stroke departments (stroke units). For patients with an intracerebral haemorrhage, however, a thrombolysis is contraindicated. The rapid diagnostic evaluation therefore plays a crucial role in stroke treatment.
In the fetal period, all three cerebral arteries are fed by the ipsilateral A. carotis interna. Once the connection of the A. cerebri posterior to the A. vertebrobasilaris arterial system is established, the original (primary) vessel atrophies and becomes the predominantly thin A. communicans posterior . However, in 20 % of the cases this does not happen, so that in adults (just like in the fetus) an A. cerebri posterior persists which is fed by the A. cerebri posterior.

Occlusions in the bifurcation area of the A. cerebri media due to arteriosclerosis or an embolism result in cerebral infarction (stroke , apoplexy) with severe deficits. These include a contralateral, predominantly brachiofacial hemiplegia with hypaesthesia (circumscribed or general decrease of touch and pressure sensations of the skin). If the dominant hemisphere is affected, this results in aphasia (speech disorder), agraphia (inability to write words and text despite having the necessary mobility of the hand, as well as the intellectual ability) and alexia (inability to read). In patients with high blood pressure (hypertension), changes in the walls of cerebral vessels can cause a vascular rupture and bleeding into the cerebral parenchyma (possibly leading to massive bleeding). The basal ganglia in particular are commonly affected by this.
Arteriosclerosis-induced changes in the wall of vessels are often found in the A. carotis interna . Small thrombi emerging from these plaques can cause an occlusion of the A. centralis retinae via the A. ophthalmica, and thus lead to a sudden painless unilateral blindness. If the thrombus dissolves within a short time it is called amaurosis fugax (short-term blindness ). As a frequent sign of cerebral circulatory disorders, it can be a red flag for an impending stroke.
 and the lateral ventricles.")
| Vessel | Origin | Flow region |
|---|---|---|
| A. choroidea anterior | A. carotis interna |
|
| Aa. choroideae posteriores | A. cerebri posterior |
|
The anterior choroid artery syndrome is caused by circulatory disorders in the area of the A. choroidea anterior and is associated with a triad of symptoms, including motor, sensory and visual dysfunctions: hemiplegia (failure of motor fibres in the Crura cerebri), hemi-sensory disorders (failure of the Crus posterius of the Capsula interna) and hemianopsia (failure of the Tractus opticus and parts of the Radiatio optica). Circulatory disorders of the A. cerebri posterior lead to visual failures, but can also be associated with temporary deficits of memory function (amnesia), as parts of the hippocampal formation are also supplied with blood from here ( Fig. 12.81 ).

The A. vertebralis can be assessed in the so-called vertebral artery triangle (→ Fig. 2.92) between the M. obliquus capitis superior, the M. obliquus capitis inferior and the M. rectus capitis posterior major; with the head bent forward, the blood flow is determined with a DOPPLER ultrasound examination.
In the case of a stroke, very unusual symptoms can develop due to the blood supply to certain regions. So it is possible that, for example, circulatory disorders of the Aa. pontis lead to failures of motor fibre tracts in ventral parts of the pons, which may be associated with an acute paraplegia. As the dorsal parts of the pons are supplied by branches of the A. superior cerebelli, important areas of awareness such as the Formatio reticularis and also the eye movements remain intact. Patients with locked-in syndrome are despite their paraplegia fully conscious without cognitive impairment, but they can only communicate with eye movements and blinking.

| Capsula interna | Arteries | Origin |
|---|---|---|
| Crus anterius | Aa. centrales anteromediales | A. cerebri anterior |
| A. striata longa (A. centralis longa [HEUBNER], A. striata medialis distalis, A. recurrens) | A. cerebri anterior | |
| Aa. centrales anterolaterales | A. cerebri media | |
| Genu | Aa. centrales anterolaterales | A. cerebri media |
| Crus posterius | Aa. centrales anterolaterales | A. cerebri media |
| A. choroidea anterior | A. carotis interna |
As the Aa. centrales anterolaterales branch off the A. cerebri media almost at a right angle, this part is particularly prone to turbulent blood flow and to secondary arteriosclerotic changes. In patients with high blood pressure (hypertension), occlusions can therefore frequently be found at these bifurcations. Occlusions as well as haemorrhages from these blood vessels can lead to tissue necrosis in the nuclear region of the cerebrum (basal ganglia) and the Capsula interna with resulting (contralateral) hemiplegia. Depending on their location, lesions of the nuclei in the cerebrum can cause severe hyperkinetic or hypokinetic disorders (dystonia).
| Artery | Topography and characteristics |
|---|---|
| A. carotis interna (ICA, internal carotid artery) |
|
| A. ophthalmica |
|
| A. choroidea anterior |
|
| A. cerebri anterior (ACA, anterior cerebral artery) |
|
| A. communicans anterior (ACOM, anterior communicating artery) |
|
| A. cerebri media (MCA, middle cerebral artery) |
|
| A. vertebralis (VA, vertebral artery) |
|
| A. inferior posterior cerebelli (PICA, posterior inferior cerebellar artery) |
|
| A. basilaris (BA, basilar artery) |
|
| A. inferior anterior cerebelli (AICA, anterior inferior cerebellar artery) |
|
| A. superior cerebelli (SCA, superior cerebellar artery) |
|
| A. cerebri posterior (PCA, posterior cerebral artery) |
|
| A. communicans posterior (PCOM, posterior communicating artery) |
|
| Vessel/vascular group | Passage | Origin | Supply area (e. g.) |
|---|---|---|---|
| Aa. centrales anteromediales | Substantia perforata anterior |
|
|
| Aa. centrales anterolaterales (Aa. lenticulostriatae) | Substantia perforata anterior | A. cerebri media |
|
| Aa. centrales posteromediales | Substantia perforata posterior |
|
|
| Aa. centrales posterolaterales | Substantia perforata posterior | A. cerebri posterior (Pars postcommunicalis) |
|
.")

Due to the blood supply in the region of the Gyrus precentralis, circulatory disorders of the A. cerebri anterior are associated predominantly with leg paralysis and circulatory disorders of the A. cerebri media with brachiofacial paralysis. The patient's clinical picture (leg or brachiofacial paralysis) therefore allows conclusions about the affected vessel.
Strokes or haemorrhages in the area of the Capsula interna frequently involve the A. striata longa (A. striata medialis distalis , A. centralis longa, HEUBNER’s artery , A. recurrens) as a branch of the A. cerebri anterior (belonging to the Aa. centrales anteromediales), or to the A. lenticulostriata as a branch of the A. cerebri media (belonging to the Aa. centrales anterolaterales) ( Fig. 12.63 ).
.")
; sagittal section.")
| Parts of the brainstem | Medial supply area | Lateral supply area |
|---|---|---|
| Mesencephalon | A. cerebri posterior |
|
| Pons | A. basilaris (Aa. pontis) |
|
| Medulla oblongata |
|
A. inferior posterior cerebelli |
| Artery | Clinical term | Cortical area | Central area | Other supply areas | Origin |
|---|---|---|---|---|---|
| A. superior cerebelli | SCA (constant) | Major part of the cerebellum, upper part of the vermis | Nucleus dentatus | Upper parts of the pons | A. basilaris |
| A. inferior anterior cerebelli | AICA (variable) | Part of the anterior cerebellar hemispheres | Lateral pons, branching of the A. labyrinthi to the inner ear in 85 % | A. basilaris | |
| A. inferior posterior cerebelli | PICA (variable) | Major part of the lower cerebellar hemispheres, flocculus | Nuclei emboliformis, globosus and fastigii | Posterior and lateral Medulla oblongata | A. vertebralis |
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here