Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

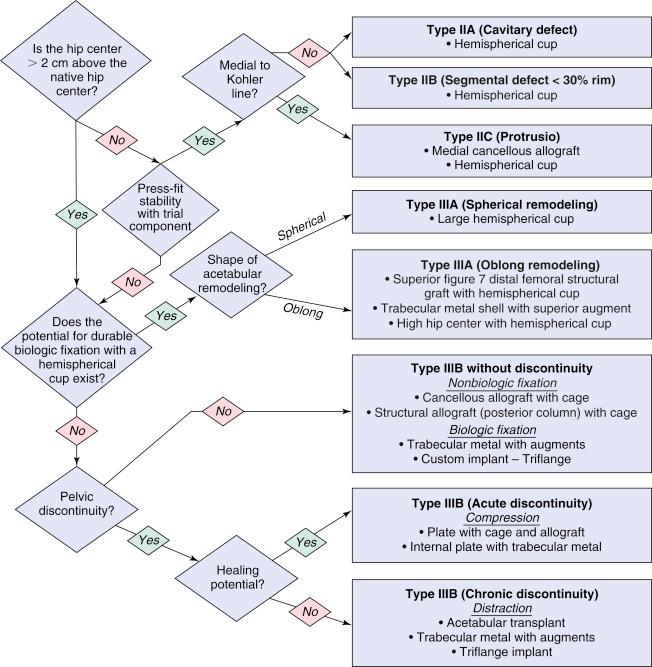
Treatment algorithm for acetabular revision proposed by Paprosky.
Numerous steps and technical issues are involved in performing an acetabular revision. Success depends on intimate contact between the implant and the remaining host bone and on creating a stable mechanical construct that minimizes micromotion, promotes bone ingrowth, and distributes the physiologic forces evenly to the surrounding acetabulum or pelvis. As in primary total hip arthroplasty (THA), the revised prosthesis must have the correct spatial orientation to avoid impingement or dislocation while restoring the hip center to its customary anatomic position to re-create normal hip kinematics. Restoration of the normal hip center requires the acetabular component to be placed as close as possible to the Kohler line and the inferomedial part of the component to be placed near the acetabular teardrop.
Preoperative planning is crucial when revising an acetabular component. Before commencing surgery, the surgeon must gain knowledge about prior surgical implants and the cause of THA failure. It is helpful to obtain serial radiographs from earlier procedures. Preoperative estimation of the volume and location of bone loss helps to determine the need for supplemental allograft bone, specialized equipment, and particular implants during revision surgery.
Fixation methods for acetabular reconstruction may be biologic or nonbiologic. Nonbiologic reconstruction relies on immediate stability of the construct without osseointegration of the component into host bone. Examples of nonbiologic techniques include cementing a polyethylene cup directly; cementing a cup with a bulk allograft, roof ring, or cage; and impaction grafting.
Biologic fixation refers to direct contact of a biologically compatible component with host bone, which promotes osseointegration and long-term fixation. Examples of this method include porous metal cups and augments (e.g., Trabecular Metal Acetabular System, Zimmer, Warsaw, Ind.). We prefer biologic fixation because of its superior durability, but osseointegration can be difficult to achieve in cases of massive bone loss. Successful osseointegration requires adequate construct stability and contact with host bone. Stable fixation with minimal micromotion (<50 μm) promotes bone formation within the pores. At least 50% surface area contact between the component and viable host bone is considered necessary for stable osseointegration. However, this value is somewhat arbitrary because the quality and location of bone and the type of metallic component used influence the minimum requirement.
Paprosky developed a treatment algorithm to guide the surgeon during preoperative planning. The choice of implant, reconstruction method, and supplemental biologic fixation depend on component migration and the extent of bone loss (see “Algorithm”). The reconstruction options described here are based on currently used implants with or without bone graft substitutes.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here