Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

An 85-year-old man presented with a painful knee 5 years after a total knee arthroplasty was performed through a limited medial incision; the posterior-stabilized prosthesis used had a modified tibial component designed for the approach with an abbreviated intramedullary stem. The laboratory workup included a culture of the joint fluid and was negative for infection. The preoperative radiographs ( Fig. 18.1 ) showed a loosened tibial tray, which was confirmed on a technetium scintigraphic study ( Fig. 18.2 ). The patient was taken to the operating room for revision. The tibial tray was loose at the time of surgery and was removed with simple manual extraction ( Fig. 18.3 ). The posterior and anterior cruciate ligaments were absent. The tibiofemoral components were revised to a constrained, posterior-stabilized design, and the original polyethylene patella was left in place. The patient had a benign postoperative course and recovered without incident.
 and lateral ( B ) radiographs of the right knee show a loosened tibial tray.")

 and the undersurface showing minimal bone loss ( B ).")
An algorith for the use of constrained implants is provided. ( CCK, Constrained condylar knee; CR, cruciate retaining; PS, posterior stabilized; TKA, total knee arthroplasty.)
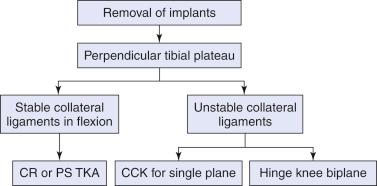
Constraint in revision total knee arthroplasty (TKA) is a balance between the stability that is present from the existing soft tissues and the stability that is afforded to the knee by the prosthetic device. The soft tissues may be lax in the preexisting knee, or they may become lax as a result of the releases that are necessary in the operating room to establish appropriate ligament balance. In the revision setting, the prosthesis must address the defects that are present due to removal of the original device and must also complement the soft tissues to produce a stable postoperative construct. Excessive constraint may lead to subsequent loosening, but laxity can lead to dislocation.
The knee that is presented for revision may include a simple unicondylar knee that has developed patellofemoral arthritis without any significant loosening, or it may be a hinge knee arthroplasty that is now loosened with significant bone loss on both sides of the joint. The choice of prosthesis for the revision must consider both the bone loss and the ligament balancing. If the collateral ligamentous structures are intact to clinical examination, a less constrained prosthesis will be adequate. If one of the collaterals is incompetent, a constrained implant will certainly be required, and if both collaterals are incompetent, a hinge will be necessary.
If the supporting collateral ligamentous structures are competent, it may be possible to implant a standard cruciate-retaining (CR) TKA (if the posterior cruciate ligament [PCL] is intact) or a posterior-stabilized (PS) TKA. In general, the PS TKA is easier to implant in the revision setting and can be used in most revision cases. As the bone loss and ligamentous support become more compromised, it is also easier to change the PS tibial insert to a constrained design.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here