Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

In the Oberg, Manske, Tonkin (OMT) classification, “Deformation” refers to disruption of a limb that has already been formed. This category previously included constriction band sequence and congenital trigger digits, although the latter has been removed in the latest OMT update.
Trigger thumbs are common. Surgical correction remains the mainstay of treatment although conservative management is increasingly practiced worldwide.
Trigger fingers are much less common. Surgical correction requires an appreciation of the anatomical anomalies that may be present, and an algorithmic strategy to treat these anomalies.
“Constriction ring sequence” refers to a wide-ranging list of conditions characterized by encircling rings to digits or limbs. A management algorithm includes early surgical release to maintain limb viability, or delayed reconstruction to optimize hand function and appearance.
“Dysplasia” refers to a group of conditions in the OMT classification which exhibit variant growth either of a hyperplastic or hypoplastic nature. Overgrowth conditions such as macrodactyly, neurofibromatosis or vascular anomalies may present as enlarged limbs or digits.
Macrodactyly is a rare and potentially disfiguring condition, usually caused by PIK3CA gene mutation in the m-TOR pathway. Strategies to optimize hand function and appearance include slowing down growth, soft tissue debulking, shortening or amputation.
 Access video content for this chapter online at Elsevier eBooks+
Access video content for this chapter online at Elsevier eBooks+
In 2013, the Swanson classification for congenital hand differences was replaced by a new system, the Oberg, Manske, Tonkin (OMT) system, proposed at the recommendation of the International Federation of Societies for Surgery of the Hand (IFSSH) Scientific Committee for Congenital Conditions. This followed growing dissatisfaction with inability of the former to classify certain conditions, such as symbrachydactyly and cleft hand, together with the rapid progression of knowledge in developmental biology and molecular genetics. The OMT system provides a logical classification system in combining etiology and morphology. The system consists of four main groups: malformations, deformations, dysplasias, and syndromes.
The OMT has undergone several changes since its original description. The “Deformation” group was initially reserved for conditions resulting from a disruption of any portion of a limb that has already been formed, consisting of constriction ring sequence (related to amniotic banding), arthrogryposis, and trigger digits. Any condition resulting from deformations or disruptions as a result of other causes, e.g., viral infection, vascular insults, or mechanical damage, was meant to be listed under the subcategory of “Not otherwise specified” or “Others”.
In subsequent modifications and updates, arthrogryposis was removed from the deformation category to “Malformation – dorsal/ventral axis” as well as “Syndromes” and then subsequently to “Dysplasia”. In the 2020 OMT update, “trigger digit” (both trigger thumbs and trigger fingers) was finally removed, due to lack of evidence that the condition is truly congenital in nature. At present, the deformation group consists of “Constriction ring sequence” and “Not otherwise specified” ( Table 36.1 ). For the purpose of this chapter, however, the conditions of constriction ring sequence and trigger digits will be discussed.
| 2010 | 2013, 2015, 2017 | 2020 |
|---|---|---|
|
|
|
Congenital trigger thumb was classified under Deformation (IIB) in the original OMT classification but was removed in the 2020 update. Considerable debate remains as to whether trigger thumb in children is a congenital condition and therefore the term “pediatric trigger thumb” will be used for the remainder of the chapter. Pediatric trigger thumb remains one of the commonest conditions faced by any practicing pediatric hand surgeon.
Pediatric trigger thumb is a stenosing tenovaginitis affecting the flexor pollicis longus (FPL) tendon as it passes underneath the A1 pulley at the volar aspect of the metacarpophalangeal (MCP) joint. The exact pathophysiology remains unknown; whether there is a pre-existing anatomical disorder that predisposes triggering, i.e., rendering it a congenital difference, is undetermined. In addition, it is also unknown why there is a much higher incidence of pediatric trigger thumb in comparison to its finger or adult counterparts.
It is a relatively straightforward task when explaining to a parent that their child has a congenital hand difference if there was an obvious hand difference at birth. However, pediatric trigger thumb is rarely encountered at birth; Kikuchi and Ogino reported an incidence of 3.3 per 1000 live births and Ger et al . mentioned an even rarer incidence of around 1 in 2000 live births. Moon et al . examined 7700 infants at birth and found no incidence of the condition. Rodgers and Waters published similar findings with 1046 infants and found no incidence of trigger thumbs, either. The proponents of a congenital theory argued that bilateral pediatric trigger thumbs have been found in identical twins. In addition, pediatric trigger thumb typically presents with a higher-than-average incidence of bilateral occurrence in non-identical twins. The question remains: why are there so many children with trigger thumbs, mostly presenting around the same age group, around 1–2 years of age, but not at birth?
One possibility is a developmental error in the vicinity of the A1 pulley at the child’s thumb MCP joint that simply predisposes to an inflammatory condition and entrapment of the FPL tendon. Another possibility is trauma, causing a narrowing of the fibro-osseous space at the level of the MCP joint. The definition of trauma remains vague; in one of the author’s (W.L.) experience involving a review of 70 consecutive trigger thumbs, 33% made their first presentation to the emergency department with “a history of trauma”, but none were subsequently found to have any injuries. Children are naturally more hypermobile and there may be a tendency for the MCP joint to hyperextend and narrow the fibro-osseous space; however, hyperextension should be a transient movement causing very little permanent effects on tendon gliding. Perhaps a combination of trauma, hyperextension in a naturally occurring tight space, can predispose some children to triggering of the thumb.
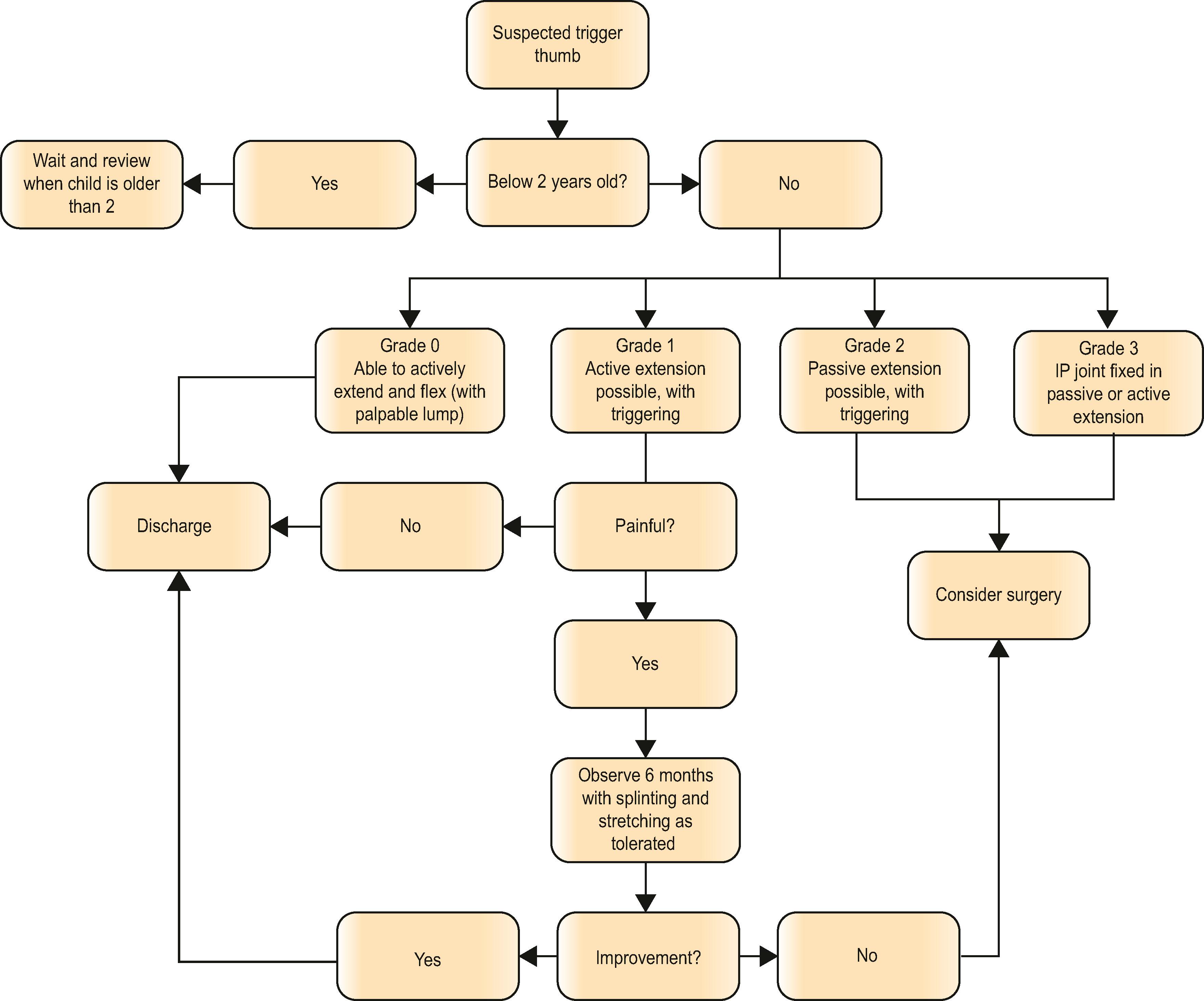
As mentioned, pediatric trigger thumb rarely presents at birth or earlier than 1 year of age, although this may reflect a failure to recognize the condition rather than its true absence. The newborn child tends to hold the thumb within the palm for months, and even to the most observant parent a deformity is only picked up when the child starts to reach out and grab objects, often around the age of 6 months. The parent notices that the child is unable to extend the thumb with the interphalangeal (IP) joint in a fixed flexion deformity, or that the child is unable to flex the thumb (an extension deformity), or that flexion and extension is accompanied by pain, or an observable “clicking” movement. Older children (above the age of 3 years) may use the contralateral hand to free the thumb. A severity score has been suggested where grade 0 implies that the IP joint can be actively extended to at least 0 degrees without triggering; grade 1where the IP joint can be extended actively but with triggering; grade 2 where passive, but not active extension, is possible, with triggering; and grade 3 where the IP joint is fixed in a flexed or occasionally an extended position. This classification is useful for communication but does not take into account symptoms of pain, which may be determinant in whether treatment is performed.
On examination, the surgeon may feel a lump in the volar aspect of the thumb MCP joint, called a “Notta’s nodule”, pathognomonic of swelling in the FPL tendon. It is important to differentiate this from a sesamoid bone, which may also feel like a prominence, but a Notta’s nodule should be more palpable and moves with flexion of the FPL tendon, unlike a sesamoid bone which remains in the same position. The examiner can also try and gently extend the IP joint passively and feel the nodule give way as the FPL tucks underneath the A1 pulley, provided this is not too painful for the child. Often, the thumb is stuck in flexion and cannot be extended, and examination can only be confirmed with palpation of a nodule and a flexed thumb. Finally, it is important to differentiate a trigger thumb from a congenital clasped thumb; the former presents with flexion deformities at the IP joint and the latter, at the MCP joint, frequently accompanied by deficiencies in the first webspace.
The obvious treatment for a child presenting with pediatric trigger thumb deformity is to “straighten the thumb” or to improve the range of movement of the IP joint. Management of a trigger thumb, however, remains controversial, for the following reasons. Firstly, is active treatment needed? Does the thumb suffer from long-term issues if it is not fully straightened? Reports of deformities in the IP joint, including contracture, radial deviation, and rotational deformity with compensatory MCP joint hyperextension and even nail deformities in untreated trigger thumbs have been reported, but these are not widely observed. Finally, the impact of the appearance of a permanently flexed thumb remains unknown, both on the parents and children.
Secondly, there are continued reports that the pediatric trigger thumb resolves spontaneously. Ger et al . observed that none of their patients demonstrated any resolution after almost 4 years of waiting; in contrast, Chalise et al . found a high rate of resolution, although this was only in stages 1 and 2, i.e., when the thumb is not fixed, and recommended a conservative approach with stretching, and surgery reserved for grade 3 trigger thumbs.
Thirdly, is surgery the best method of treatment? Since Jahss prioritized surgery as the only treatment for trigger thumbs, there has been a recent move towards conservative management. A resolution rate of about 30% has been reported if the child presents before 1 year old, but this dramatically decreases as the child gets older. Watanabe et al . recommended a conservative approach in grades 1 and 2 but surgery in grade 3 and reported a final satisfactory rate of 96% with abnormal motion in about 59% of thumbs. Finally, Baek et al . reported a spontaneous resolution rate of >75% after a follow-up of at least 5 years; in the remaining 25%, there was at least some improvement. They admitted that fine motor movement may be adversely affected by an incomplete resolution and recommended waiting until 5 years of age to decide surgery, but not beyond that. Tan et al . found a high success rate with conservative treatment, especially in very young children, but attributed it to the use of splints. Finally, Lee et al . recommended splinting with good results but cautioned that not all thumbs would regain normal movement.
A cursory glance at the literature would perhaps reveal an East–West divide, with conservative management favored in Asian countries but surgical release in Western ones. The higher rate of success with conservative management in the East may be attributable to the increased hypermobility in children or other cultural factors, including compliance. Overall, the indications for surgery would therefore appear to be a child presenting after the age of 2 and before 5, with a fixed flexion (or extension) deformity, or an intermittently triggering thumb that is painful. A desire for a full correction of the IP joint, for whatever reasons, including appearance, may be another indication (see Algorithm 36.1 )
To ensure optimal visualization of the A1 pulley and protection of the neurovascular bundles, avoid rotation of the thumb during surgery or assistance.
Draw a line in the longitudinal axis of the thumb as a reference to keep orientation during surgery.
Ensure adequate distal and proximal release of the A1 pulley and check excursion of the flexor pollicis longus (FPL) tendon after release.
Do not excise Notta’s nodule on the FPL tendon.
Be aware that the thumb may not achieve a symmetrical position to the normal contralateral thumb, especially if it has been flexed for a long time.
Preoperatively, in unilateral cases, it is important to warn parents that the thumb may not straighten to the same degree as the contralateral normal one. Children often present with a naturally hyperextended MCP joint and this often-overlooked posture should be made known to the parent. Once released, however, the IP joint thumb extension should eventually approach that of the normal side over time.
 Transverse crease incision. (B) Release of A1 pulley, initially with scalpel and then with scissors. (C) Check for full tendon excursion after pulley release. (D) Postoperative appearance at 3 months showing a completely straight left thumb with full range of motion.")
Surgery is typically carried out as a general anesthetic day case, under tourniquet control and loupe magnification. A transverse incision is preferred rather than a Bruner one, situated at the base of the thumb. There are usually three naturally occurring thumb creases and the incision is placed in the center one. It is helpful to mark the midline axis of the thumb for reference, as rotation of the thumb can easily occur during assistance and inadvertently displace the digital nerves into the center of the operative field ( ). The initial incision is kept superficial, sufficient to visualize the initial appearance of fat and the rest of the dissection performed with tenotomy scissors. Once the proximal edge of the A1 pulley is visualized, a longitudinal window is made in the pulley with a scalpel, until the FPL tendon fibers are visualized, and the rest of the pulley release is completed distally with scissors. The use of a blunt retractor should allow direct visualization of the divided pulley, which would appear as a “V”, with the apex situated distally. The tips of the scissors are then inserted and under direct observation, the last fibers of the A1 pulley are divided, and the cut edges should appear parallel to each other. The direction of release should be kept in the midline to avoid damaging the digital neurovascular bundles, although some surgeons prefer to keep it slightly radial, to avoid cutting the origin of the oblique pulley. However, a slightly radial release must be balanced with the risk of damaging the radial digital nerve, which usually lies in a more midline position during surgery. Once released, the IP joint should straighten naturally but as mentioned, the degree of extension may not immediately be identical to the contralateral thumb. However, the IP joint should move freely without any evidence of triggering at this stage and a passive tenodesis test should produce full IP joint extension. A skin hook retractor is then used on the lower skin edge to allow visualization of the proximal part of the wound and to release any existing tight bands.
The FPL tendon is then retracted out of the wound to check for full excursion and to break up any adhesions. Notta’s nodule is observed and, if present, no attempts should be made to excise it, as this would cause more inflammation. Wound closure is achieved with interrupted 6-0 Vicryl Rapide sutures. The hand is dressed with the thumb extended, and the tip exposed in an older child and a full boxing glove in a younger child.
The wound is checked at 2 weeks and dressings removed to usually reveal a straight thumb that can move freely. Before removal of dressings, the parents are warned again that the posture of the thumb may not be identical to the other. Physiotherapy is very rarely required as the child makes full use of the thumb immediately. The child is then seen at 3 months postoperatively, and very often, the posture of the operated thumb is observed to be symmetrical to the other.
The outcome of surgery is usually excellent, in all aspects including parental satisfaction for scar, pain, and ease of care. The overall incidence of complication is around 1–2%, mainly in the area of wound infections. Occasionally, there is residual triggering, or the thumb remains in a flexed position, and the common reasons are inadequate release or tendon adhesions, and a period of splinting should be allowed to see if the condition improves. There is perhaps a higher incidence of true recurrence in children with more hypermobility but evidence for this is lacking.
If there is true recurrence or if the thumb remains stuck in flexion, a trigger release can be performed in the same manner. However, imaging investigations are recommended to ensure there are no other pathologies that may account for the triggering.
The incidence of pediatric trigger finger is about ten times less common than its thumb counterpart, and much rarer as compared to its adult counterpart. There remains a paucity of evidence about its etiology and the best way to treat this condition. As mentioned, trigger digits have recently been removed in the most recent update of the OMT classification over controversies as to whether this is an acquired or congenital condition.
Like trigger thumb, there is little evidence of pediatric trigger finger being present at birth. They have been reported in children as early as 3 weeks, with the majority presented before 8 months of age. Despite its unknown etiology, however, most authors reported recurrent anatomical anomalies accounting for the triggering, which may support the case for a congenital cause. Schaverien and colleagues classified the anatomical anomalies into three groups: (1) tendon anomaly (tendon nodules, wide flexor tendons); (2) abnormal relationship between the flexor digitorum superficialis (FDS) and profundus (FDP), such as a proximal or narrow decussation of FDS or aberrant connections between the flexor tendons; and (3) narrowing of the pulley system which can affect A1, A2 or A3 pulleys. A plausible causative explanation can therefore be a child born with these predisposition anatomical anomalies, presenting with a trigger finger following a subsequent “acute on chronic” event. Rarer conditions that can also increase the contents of the sheath and cause triggering include inflammatory synovitis from juvenile rheumatoid arthritis, post-traumatic calcific tendonitis, benign osteochondromas or mucopolysacchariodosis type 1 (Hurler’s syndrome). If there is any evidence of systemic involvement, referral to a rheumatologist is warranted. Radiographs are unlikely to be helpful, but ultrasound examination may reveal the underlying etiology and location of entrapment.
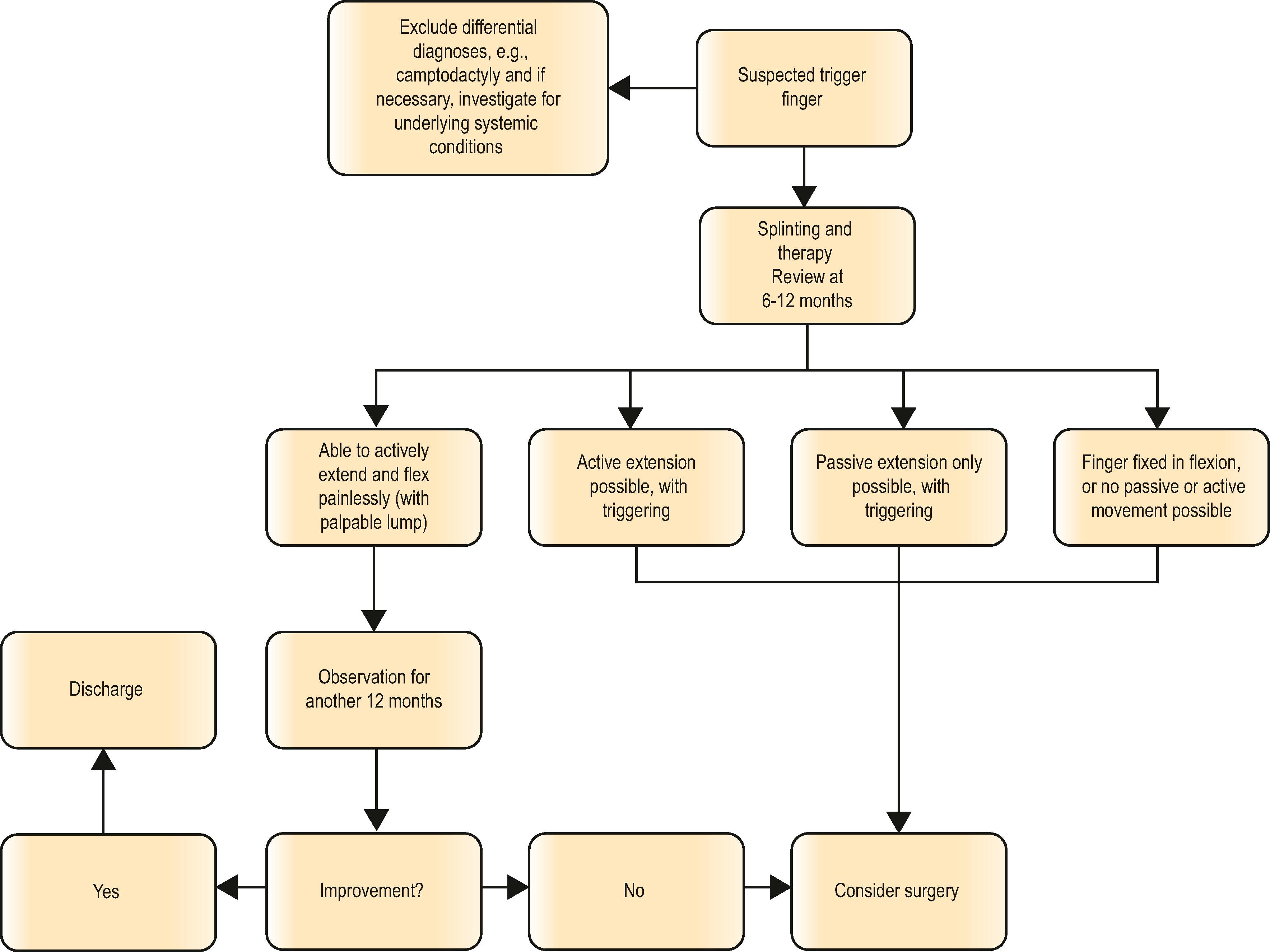
Although patients with pediatric trigger finger can present early, the age of presentation is usually slightly older, as compared to pediatric trigger thumb. One or more digits may be affected, although the middle is the commonest. Other important differential diagnoses to exclude include camptodactyly or aberrant muscles of the forearm, including isolated congenital deficiency of the extensor mechanism or contracture of the long flexors. Camptodactyly-arthropathy-coxa vara-pericarditis syndrome (CACP) is a rare autosomal recessive condition which can present with multiple fixed flexion contractures, in which surgery should be avoided. On physical examination, the child may present with a persistently flexed digit when attempting to open the hand, while others demonstrate a decreased active range of motion, or normal range with frank triggering, which may be painful or painless. An older child would often use the other hand to open the digit. A Notta’s nodule, similar to that found in trigger thumbs, can often be palpable in the region of the A1 pulley. An abnormally proximal FDS decussation can similarly be felt as a prominence traveling under the A1 pulley, as the finger flexes and extends.
There are fewer specific data on the non-surgical management of pediatric trigger finger as compared to trigger thumb, in part due to the grouping of both conditions in earlier publications. Bae et al . observed patients for a minimum of 6 months to determine if spontaneous resolution might occur, except in those who presented with locked digits. The systematic review by Womack et al . reported a total of 64 digits that received initial nonoperative treatment, with resolution in 37 triggering digits (57.8%). A period of observation for 6 months to a year is probably reasonable, unless the child reports pain or functional limitations, or if the other hand is constantly required to help release the digit. Unlike adults, a corticosteroid injection cannot be routinely administered in younger children because of the reduced tolerance to pain and injection.
Trigger finger is an uncommon condition in children. Exclude any systematic associations and if in doubt, refer to a pediatric rheumatologist.
Use a Bruner incision with extensile options to expose A1–A4 pulleys.
Release A1 pulley first and check for excursion of the flexor digitorum superficialis (FDS) and profundus (FDP) tendons. If triggering persists, check for distal pathology.
If necessary, excise one slip of the FDS tendon to ensure free gliding of both FDS and FDP postoperatively.
If recurrence occurs, consider undiagnosed systemic cause or imaging modalities to exclude other anatomical reasons for triggering.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here