Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

 Access video lecture content for this chapter online at Elsevier eBooks+
Access video lecture content for this chapter online at Elsevier eBooks+
Breast reconstruction with autologous tissue transfer is an option for patients following unilateral or bilateral mastectomy. To date, approximately 26% of women in the UK undergo autologous reconstruction following mastectomy. The diversity of techniques available, each with its own indications and benefits, make it possible and essential to treat patients tailored to their individual preferences and body shape. Depending on the patient’s anatomy, autologous tissue can be harvested from different regions that include the abdomen, thigh or buttock. The ultimate aim to be achieved, however, regardless of donor area, is to restore the resected breast tissue with something similar in terms of shape, size and quality. Women should postoperatively have the sensation of a natural appearing breast, both visually appealing, as well as to the touch.
When the first stage of reconstruction is achieved, further refining procedures generally follow to improve and enhance cosmetic results. Revisional surgery may include the reconstructed breast, contralateral breast, or both. The main goal in unilateral cases is the creation of ideal symmetry with regards to the unoperated contralateral breast. This status can be achieved in various ways, either with or without balancing surgery to the opposite healthy breast. The decision to perform symmetrization surgery on the contralateral breast has to be thoroughly evaluated, as many factors influence the decision. The prospect of having surgery on an otherwise healthy breast can sometimes be intimidating to the already physically and psychologically troubled patient. Other patients might profit from balancing surgery due to symptomatic macromastia, significant breast hypoplasia or a ptotic breast, and would have chosen to undergo plastic surgery regardless of breast cancer diagnosis. Choices for refinement surgery are made based upon patients’ expectations regarding symmetry, breast contour, volume, position and aesthetic outcome. In bilateral cases it is often easier to decide which secondary procedures are necessary: a nice shape and symmetry of both breast mounds should be strived for, with a size and form suiting the patient’s figure.
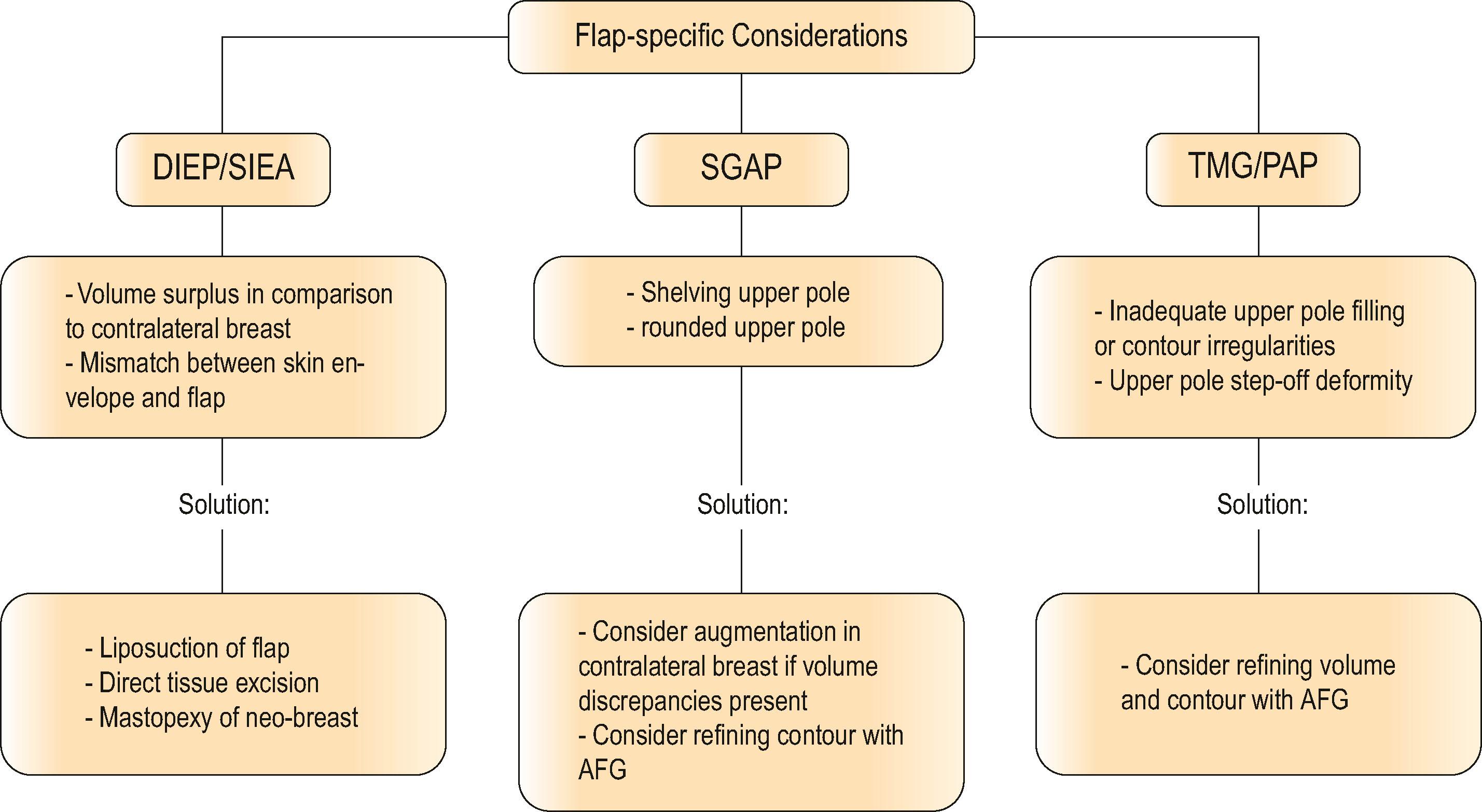
There is no “one procedure fits all” concept in secondary surgery after autologous breast reconstruction. Depending on the flap chosen, the necessary touch-ups differ slightly. For example, in abdominally based flaps, the most commonly chosen flap type, volume discrepancies are often encountered and adjusted. In gluteal flaps where the transferred tissue is fairly rigid, a sharp transition to the chest wall (shelving) develops and is corrected. Also, in these cases, the contralateral breast occasionally needs augmentation to mimic the rounded upper pole of the neo-breast.
In thigh-based flaps, autologous fat grafting for minor irregularities are frequently useful. These secondary corrective procedures focus on the breast. However the donor site should not be neglected, as outcomes may turn out aesthetically unfavorable.
In short, the secondary procedures required can be divided into five categories:
Volume correction of neo-breast (augmentation/reduction)
Correction of contour and structural irregularities
Reconstruction of nipple–areolar complex (NAC)
Symmetrization of contralateral breast
Corrections to donor site.
Regardless of chosen flap type, it is of utmost importance that the patient is aware of the various stages of breast reconstruction, before entering on the journey. In general, the initial reconstruction with vascularized tissue transfer indeed offers a pleasing aesthetic result, but it is only the primary step in achieving a complete breast reconstruction. Regardless, selection of flap type, the transferred tissue undergoes changes and naturally adapts to the surrounding chest wall. In doing so, the volume, shape and position of the transferred tissue is altered over time. Therefore, secondary procedures should ideally be scheduled after completion of transformation, and the reason communicated and exactly explained to the patient. The aim should be to give women an approximate time schedule on the expected procedures, as soon as possible during initial consultation. Some patients may not want to go ahead with corrective surgery, and are content with the result after one single operation. One should note the difference between patients and surgeon’s satisfaction, being attentive not to push women into a second procedure against their will.
In order to assess if further surgical corrective procedures are needed to the ipsilateral and contralateral breast, patients are evaluated 3 months after the initial autologous reconstruction. This time span allows the tissue to settle, and any swelling or minor fluid accumulation to subside. In this setting, the breast symmetry can be addressed more precisely. Others may prefer to perform the symmetrization during immediate reconstruction, and in doing so use the adjusted contralateral side as a model for flap shaping. It is of our opinion however, that the changes taking place postoperatively make an immediate symmetrization less predictable.
Typically, weight fluctuations take place after diagnosis of breast cancer with a trend toward weight gain in the long term. The corrective surgeries should first take place when a steady state is reached. This allows for a sustainable long-term result and reduces the risk for additional corrective procedures.
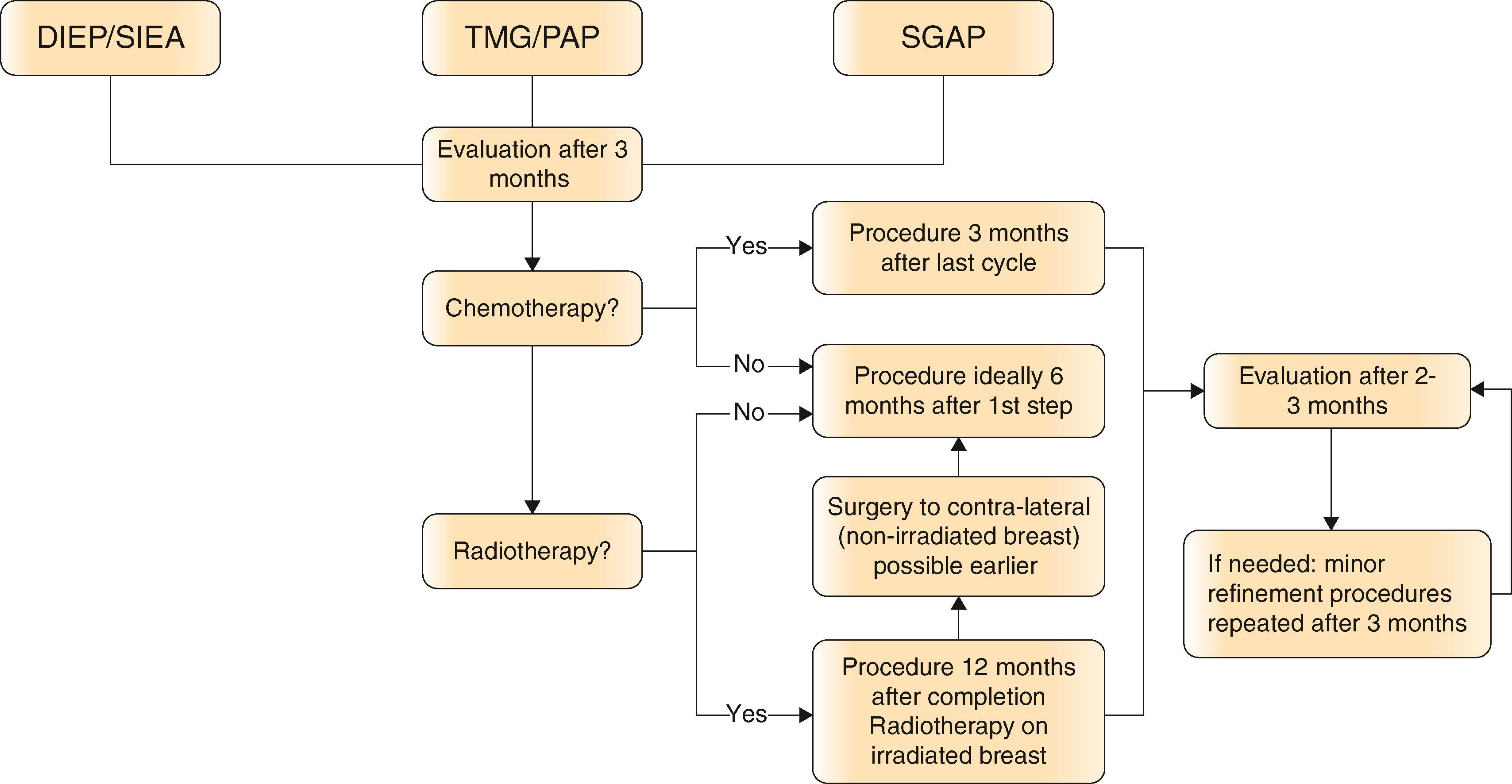
Following mastectomy and immediate reconstruction, the oncological decision for further adjuvant therapy should be rendered within 3 months. Providing that no chemotherapy or irradiation is needed, the optimal timing for secondary procedures begins at 6 months. The corrective operations are typically not carried out during chemotherapy, but rather after patients have recovered, usually 1–3 months after the last cycle. In cases needing irradiation, our approach is to wait at least 1 year after completion of the therapy before conducting surgery on the irradiated breast ( Algorithm 43.1 ). Effects of irradiation on the transferred tissue leading to poor aesthetic outcome include fibrosis, contracture and hyperpigmentation. Also, the potential for reconstruction-threatening complications tend to occur within the first year of irradiation and decreases significantly with time. In cases needing only a symmetrization of the contralateral side, the surgery can be scheduled at an earlier point in time.
There is also an additional reason for waiting with corrective procedures concerning the neo-breast. When transferring autologous tissue, the microcirculation of the flap is altered. Early refining surgeries to the flap tissue might impede flap perfusion significantly. Therefore, an interval of 6 months should pass before touching the ipsilateral side without fear of compromising flap viability.
After a first corrective procedure, a new evaluation is carried out approximately 2–3 months later. If further refinements are necessary, these can be carried out relatively quickly after stabilization and complete healing. This sequence can be continued until a satisfying result is achieved (see Algorithm 43.1 ).
During patient counseling the individual wishes should be identified and addressed. In order to define the exact surgical planning, patients are asked to pinpoint three aspects which are bothering and can be tackled. These points may vary from the treating surgeons’ thoughts and ideas. Most of the time, however, patients and surgeons alike wish to accomplish best possible symmetry.
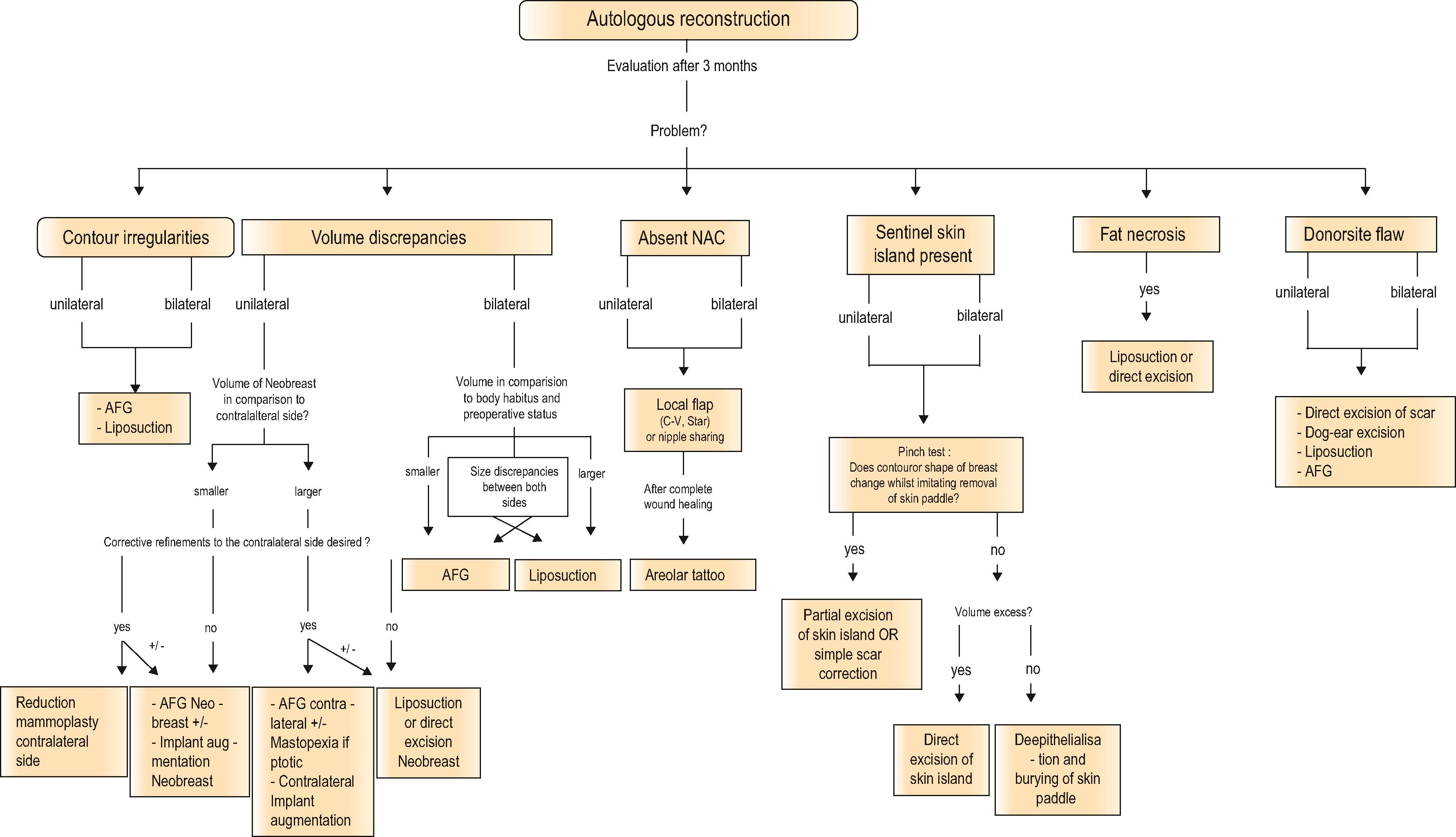
A surgical plan is developed together with the patient depending on the selected flap, clinical status and patient’s wishes. Selecting the optimal treatment strategy can be achieved after identification of the main problem(s) ( Algorithm 43.2 ). For each flap there is a slightly differing treatment algorithm, concentrating on the specific issues linked with the characteristics of transferred flap tissue and donor site ( Algorithm 43.3 ).
Markings are carried out on the standing patient, putting meticulous emphasis on the symmetry to both sides. This is critical to maximizing the symmetry, especially in cases of irradiated tissue, as it tends to be rigid and shows other aspects than natural breast parenchyma. Contour abnormalities or volume discrepancies requiring treatment are carefully marked in order to treat correct areas intraoperatively. In the operating room, the patients are placed in a prone position, with the possibility of a seated position (almost 90°) on-table. The majority of procedures are conducted under general anesthesia in an outpatient setting.
A frequent reason for revisional surgery is an existing volume disproportion. In unilateral breast reconstructions volume asymmetry can be the result of a flap that is too large or too small to match the opposite breast; in bilateral breast reconstructions volume discrepancies may arise in comparison to preoperative breast size and shape. On the one hand, the problem can be a total excess or deficiency of volume, usually due to the initial correlation between the flap volume and the skin envelope in the primary reconstructive procedure. In cases with an abundance of skin and relatively sparse flap tissue, breast shape becomes ptotic. In contrast, when flap volume is high and skin volume almost insufficient, the breast mound appears compact and elevated following the reconstructive procedure. Normally, autologous breast reconstructions are created slightly larger than the opposite breast, with the anticipation that the volume will decrease over the first couple of months after surgery. If this is not the case, refining procedures follow.
On the other hand, volume loss or surplus can also appear to be localized in different breast quadrants, usually due to a certain initial insetting and shaping of the flap. Especially in bilateral cases the options of flap shaping are limited due to the given shape of the hemi-abdomen, which can result in a breast mound without desired projection, cleavage and lateral contour. Another reason for localized volume deficiencies may be the result of partial flap loss. In a few cases the symmetry and overall appearance of the breast mound might seem appealing; however, patients complain of a volume excess in the lateral area. This is the case when the thoracodorsal pedicle is used as a recipient vessel, and a surplus of lateral flap tissue results due to flap positioning.
The various problems concerning volume incongruities can be summed up in two categories:
Total volume excess/deficiency
Partial volume excess/deficiency.
The aim of final breast mound shaping is to refine the size and shape, using various techniques as a means to sculpt the reconstructed breast. The main surgical tools include volume supplementation (autologous fat grafting) and volume reduction (liposuction and direct tissue resection). When there is a severe lack of volume in unilateral cases, either on the reconstructed or natural side, augmentation with an implant is a possibility to correct size inequality. These mentioned techniques can either be combined or used independently to achieve a satisfying result.
After autologous breast reconstruction, using either abdominal, gluteal or thigh-based tissue, contour abnormalities may occur. In most cases this can either be readily addressed by suction-assisted lipectomy of the subcutaneous tissues, or approached with autologous fat grafting in the area needed. Indentations, which can occur after partial flap necrosis, and unpolished contours are standardly treated with injection of fat tissue. Especially in gluteal-based flaps, it is regularly difficult to achieve a smooth transition to the surrounding tissue of the flap. Classically, a step-off in the upper and medial quadrants at the interface between neo-breast and chest wall is seen ( Fig. 43.1 ). In these cases, autologous fat grafting can provide a remedy.
 A 46-year-old patient with bilateral carcinoma of the breast and asymmetry. (B) 3 months following bilateral skin-sparing mastectomy (SSM) and primary autologous reconstruction with superior gluteal artery perforator flap. Secondary procedures planned after 6 months: autologous fat graft to both upper poles; bilat. nipple–areolar complex reconstruction. (C) Follow-up at 3 months after fat grafting (40 cc right side;150 cc left side) and areolar tattooing.")
The occurrence of fat necrosis, a well-recognized sequela, can compromise a breast reconstruction by causing firm to hard areas of the reconstructed breast that are not as soft or mobile as natural breast tissue. These areas can either be treated with suction-assisted lipectomy or direct excision. The latter technique, however, may result in an undesirable contour deformity and should be conducted with caution. Afterwards, in a second revision, fat grafting may be needed to treat the developed indention.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here