Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Undisplaced fracture of distal radius.
Dislocation involving the lunate.
Greenstick fracture.
Triquetral fracture.
PA , Lateral , Scaphoid series .
AVN, avascular necrosis; C, capitate; L, lunate; PA, posterior-anterior (view); R, radius.
The articular surface of the radius lies distal to that of the ulna in 90% of normal people.
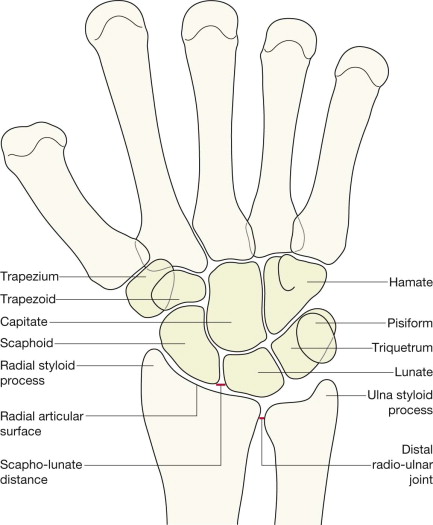
The carpal bones are arranged in two rows, bound together by strong ligaments:
The joint spaces are uniform in width: 1–2 mm wide in the adult.
Adjacent bones have parallel/congruous surfaces.
Abnormally narrow spaces are invariably due to radiographic projection or to age related degenerative change; rarely due to injury.
Abnormally wide spaces are likely to indicate damaged ligaments.
The dorsal cortex of the distal radius is completely smooth—no crinkles, no irregularity. This cortex should be as smooth as a baby's bottom.
The alignment of the carpal bones may appear confusing but identifying the important anatomy is actually very simple. Don't worry about the overlapping bones. Just think: apple, cup, saucer.
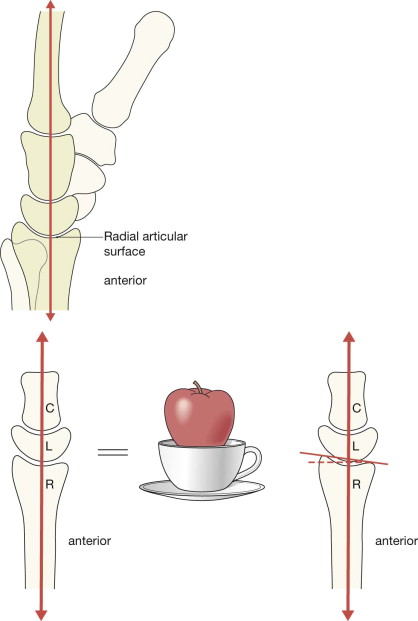
The distal radius, the lunate and the capitate articulate with each other and lie in a straight line; like an apple in a cup sitting on a saucer. The radius (R, the saucer) holds the lunate (L, the cup) and the cup of the lunate contains the capitate (C, the apple).
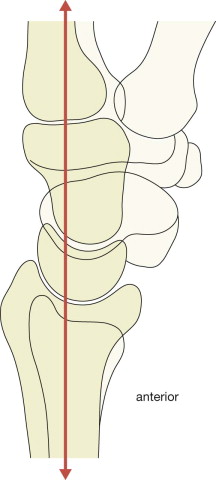
The articular surface of the radius has a slight but definite palmar (ie anterior) tilt. The angle of tilt is usually about 10°, but ranges from 2° to 20°.
The PA view will appear fairly comforting to an inexperienced observer because all of the carpal bones are clearly shown. The lateral radiograph may appear terrifyingly complex and difficult to analyse because of the numerous overlapping bones. There is a very clear message: do not be afraid!
The lateral view is diagnostically very, very, important, so we will show you how to quickly and confidently analyse every lateral radiograph using a simple checklist.
Analysis : ask yourself five questions.
Questions 1–4 apply to all adults. Question 5 applies to all children.
Is the radial articular surface and/or the ulna styloid process whole and intact?
No = undisplaced fracture.
Does the radial articular surface lie distal to the ulna?
No = suspect disruption at the radio-ulnar joint.
Is the scaphoid bone intact and normal?
No = fracture.
Is the scapho-lunate distance less than 2 mm wide?
No = suspect a tear of the scapho-lunate ligaments ( p. 147 ).
In children: does the radial cortex show any angulation or any suggestion of a localised bulge?
Yes = Greenstick or Torus fracture.

A subtle lucent line crosses the metaphyseal–diaphyseal region of the radius.
Note the slight bulging of the adjacent cortex.
Fracture of the radius. A Torus fracture ( p. 18 )
Analysis : ask yourself five simple questions on each and every lateral view. No exceptions.
If you ask and correctly answer these five questions you will detect all the subtle and clinically important abnormalities.
Is the radial articular surface intact?
No = undisplaced fracture.
Is the dorsal cortex of the distal radius smooth? Specifically:
Is the cortex as smooth as a baby's bottom?
No crinkle, no angulation, no bulge, no buckling?
Are you sure? Check the dorsal cortex one more time.
No, it is not smooth = undisplaced fracture.
Is the palmar tilt (normal range 2–20°) of the articular surface of the radius normal?
No = suspect an impacted fracture.
Is there a bone fragment lying posterior to the carpal bones?
Yes = Triquetral fracture.
Is there a bone sitting in the cup of the lunate?
No = carpal dislocation involving the lunate ( pp. 148–150 ).
Many undisplaced scaphoid fractures are not visualised on the two standard (wrist) views. Two extra views produces a better return. Therefore, a four view scaphoid series is essential and should be requested whenever there is ‘snuffbox’ tenderness:
The two additional images will vary between Emergency Departments. Importantly, two of the four projections will always include a true PA and a true lateral of the wrist.
Scaphoid fractures are mainly hairline fractures and lucent; they are not sclerotic. Occasionally the fracture is displaced.
Analysis : ask yourself three questions.
Does the scaphoid appear intact on each of the four views?
No = fracture (see p. 144 ).
Is the distal radius—particularly the styloid process—intact?
No = fracture (see pp. 136–141 ).
AND
Have I checked the PA and lateral views step-by-step (see pp. 128–130 )?
No = start checking.
Inevitably there will be some soft tissue swelling over the site of an injury due to simple bruising, a ligamentous injury, a fracture, or a combination of all of these. This soft tissue swelling on the radiograph is not particularly helpful in terms of radiological diagnosis. There have been claims that the appearance of some soft tissue fat stripes around the wrist can be helpful, but this is not the case .
| Age (years) | Very young (4-10) | Older children (10-16) | Young adults (17+) | Middle age (50+) | Elderly |
|---|---|---|---|---|---|
| Usual fracture | Greenstick or Torus | Epiphyseal (Salter– Harris) | Scaphoid or Triquetal | Colles' | Colles' |
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here