Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Following a head injury the imaging examination of choice is CT .
Plain film skull radiography (SXR) has in the main been abandoned or its use radically reduced as a first line imaging test both in children and in adults .
A SXR is now limited to:
where national or local guidelines indicate a role within a patient management algorithm;
locations where imaging resources are limited and CT is not available.
If a SXR is obtained there are just three abnormal features to look for: linear fractures, depressed fractures, and a fluid level in the sphenoid sinus.
Radiographs comprising a standard SXR series:
A Lateral obtained with a horizontal X-ray beam, and one additional view depending on the site of injury.
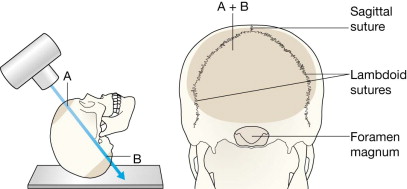
Trauma to the occipital bone
= Towne's view .
Any other injury
= PA frontal view .
CT, computed tomography; PA, posterior-anterior view; SXR, skull X-ray.
Following an apparently mild head injury requests for skull radiography (SXR) will occur very infrequently . Compelling evidence that CT should be the examination of choice was initially based on a meta-analysis of 20 head injury surveys . SXR series may still be requested, perhaps in remote locations where imaging facilities are limited.
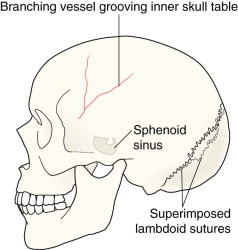
Most difficulties with interpretation arise because a normal appearance can be mistaken for an abnormality. These false positive diagnoses can be reduced by being familiar with the following.
The normal sutures and accessory sutures ( pp. 36–39 ). Specifically, the position and appearance of:
the three large sutures: the lambdoid, coronal and sagittal;
the other smaller sutures around the mastoid bones.
The metopic suture ( p. 38 ). The most common accessory suture persisting in some adults.
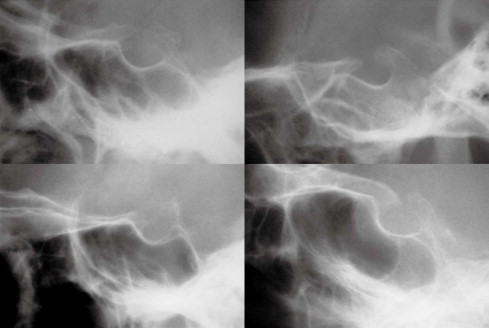
Vascular impressions. Specifically:
the sites of the most common vessel grooves/markings;
the radiographic features ( p. 52 ) that help to distinguish between a fracture and a vessel marking.
The normal sphenoid sinus.
In young children it is not pneumatised.
In adults it contains air. The variable pneumatisation causes the radiographic appearance to differ widely between individuals.
In practice, the detection of a SXR abnormality is easy. There are really only three findings/abnormalities that indicate that a fracture is present—and one of these is very rare. The radiographs need to be checked/inspected in a systematic manner.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here