Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The first comprehensive classification of nervous system tumors, formulated by Percival Bailey and Harvey Cushing in 1926, was founded on presumed parallels between embryologic and neoplastic cells. In large part, this histogenetic “cell of origin” model still forms the basis for today's nomenclature, although much of the terminology has changed considerably. Renewed interest in the role of developmental pathways in tumorigenesis has led to more recent studies focusing on cancer stem cells and progenitor cells, as well as in disease-defining driver mutations. In 1949, as a means of enhancing the clinical utility of tumor classification, Kernohan contributed a tumor grading system focusing on correlations with patient prognosis. As progress was made over time, Russell and Rubinstein continued to modify and update the Bailey and Cushing system from the 1960s through the 1980s. Nonetheless, considerable variability in diagnostic practice existed on both sides of the Atlantic Ocean. In order to enhance consistency, an experts' consensus scheme known as the World Health Organization (WHO) classification scheme was first completed in 1979 and then revised in 1993, 2000, 2007, and 2016. This latter scheme is now the most widely utilized by neuropathologists for tumor typing and grading.
The 2016 WHO “blue book” currently lists over 100 types of nervous system tumors and their variants. It also departs from prior editions in being the first to integrate molecular criteria into the definitions of many adult and pediatric tumor types. This level of complexity can be daunting; therefore, an organized approach or algorithm is required. As a first step, consideration of clinical and radiologic characteristics is a critical way to narrow the differential diagnosis, often to a few fairly common entities. In fact, the combination of patient age and neuroimaging features (including tumor location) provides some of the most powerful diagnostic clues before any tissue is even sampled or examined under the microscope. For example, the differential varies considerably for supratentorial versus infratentorial, pediatric versus adult, and enhancing versus nonenhancing tumors. The most common diagnostic considerations are therefore summarized by age, location, and imaging features in Table 1.1 , with each specific entity discussed in greater detail in subsequent chapters. Also, for a much more detailed background on the use of neuroimaging, the reader is referred to Chapter 4 , while the more recent approach of using classic molecular patterns/profiles as a diagnostic aid is summarized in a completely new Chapter 5 . Radiology is a particularly critical topic in surgical neuropathology, since brain and spinal cord biopsies are often small and the neuroimaging essentially provides the “gross pathology.” At the opposite end of the pathology spectrum (i.e., submicroscopic), molecular alterations are increasingly providing diagnostic, prognostic, and/or predictive data that are essential for the daily care of brain tumor patients. Therefore, the reader must be aware of their burgeoning roles in routine neuropathology and practical ways to integrate these new genetic and genomic algorithms.
| Location | Child/Young Adult | Older Adult |
|---|---|---|
| Cerebral/Supratentorial | Ganglioglioma (TL, cyst-MEN, E) DNT (TL, intracortical nodules) PXA (TL, cyst-MEN, E) CNS embryonal neoplasms (solid, E) Ependymoma (solid, E) AT/RT (infant, E) |
WHO grades II–III diffuse glioma (NE, focal E) GBM (E or rim E, butterfly mass) Metastases (grey-white junctions, E or rim E) Lymphoma (periventricular, E) |
| Cerebellar/Infratentorial/Fourth ventricle | PA (cyst-MEN) Medulloblastoma (vermis, E) Ependymoma (4th v., E) Choroid plexus papilloma (4th v., E) AT/RT (infant, E) |
Metastases (multiple, E or rim E) Hemangioblastoma (cyst-MEN) Choroid plexus papilloma (4th v., E) |
| Brainstem | PA (dorsal, exophytic, cyst-MEN) DMG, H3 K27M mutant (pons, ±E) |
Diffuse glioma/Gliomatosis cerebri (multifocal, ±E) Metastases (multiple, E or rim E) |
| Spinal cord (intramedullary) | Ependymoma (E, ±syrinx) PA (cystic, E) DMG, H3 K27M mutant (expansile, ±E) Drop metastases (cauda equine, E) MPE (filum terminale, E) |
Ependymoma (E, ±syrinx) DMG, H3 K27M-mutant (expansile, ±E) MPE (filum terminale, E) Paraganglioma (filum terminale, E) |
| Spinal cord (intradural, extramedullary) | Clear cell meningioma (±dural tail, E) Schwannoma (NF2, nerve origin, dumbbell shape, E) Drop metastases (leptomeningeal, E) Melanocytoma/melanoma (E, meningeal based) |
Schwannoma (nerve origin, dumbbell shape, E) Meningioma (±dural tail, E) Melanocytoma/melanoma (E, meningeal based) MPNST (±NF1, E, necrotic) |
| Spinal cord (extradural) | Bone tumor spread (EWS, usually E) Meningioma (±dural tail, E) Abscess (E) Vascular malformations (dilated vessels on imaging, ±E) |
Herniated disc (T1-spin echo, NE) Postoperative scar (E) Secondary lymphoma (E) Metastases (E) Abscess (E) |
| Extra-axial/Dural/Leptomeningeal | Secondary lymphoma/leukemia (E) Meningeal rhabdomyosarcoma (E) EWS (E, ± dural tail) DLGNT (diffuse meningeal E, ±intraventricular masses) Meningeal gliomatosis CSF dissemination of medulloblastoma or CNS embryonal tumor (drop mets or diffuse meningeal E) |
Meningioma (E with dural tail) SFT/HPC (E with dural tail) Metastases (E) Secondary lymphoma/Leukemia (E) Marginal zone lymphoma (E) Rosai-Dorfman disease (E) IgG4 disease and collagen vascular disorders (E) Meningeal carcinomatosis, melanomatosis, sarcomatosis, lymphomatosis, or hemangioblastomatosis (diffuse meningeal E) |
| Intrasellar | Pituitary adenoma (solid, E) Craniopharyngioma (cystic, E) Rathke cleft cyst (cystic, ±E) Pituicytoma/SCO/GCT (solid, E) |
Pituitary adenoma (solid, E) Craniopharyngioma (cystic, E) Rathke cleft cyst (cystic, ±E) Pituicytoma/SCO/GCT (solid, E) |
| Suprasellar/Hypothalamic/Optic pathway/Third ventricle | Germinoma/MGCT (E) Craniopharyngioma (cystic, E, Ca + ) PA (cyst-MEN) Pilomyxoid astrocytoma (infant, solid, E) Langerhans cell histiocytosis (E) |
Colloid cyst (3rd v., ±E) Craniopharyngioma (cystic, E, Ca + ) Chordoid glioma (anterior 3rd v., E) |
| Pineal | Germinoma/MGCT (solid, E) Pineocytoma (solid, E) PPTID (solid, E) Pineoblastoma (solid, E) Pineal cyst (cystic, NE) |
Pineocytoma (solid, E) PPTID (sold, E) Pineal cyst (cystic, NE) |
| Thalamus | PA (cyst-MEN) DMG, H3 K27M-mutant (E, NE) |
DMG, H3 K27M-mutant (E, NE) GBM (rim E) Lymphoma (E, ±multifocality) |
| Cerebellopontine angle | Vestibular schwannoma (NF2, E, involves internal auditory meatus) Choroid plexus tumor (E, component in 4th v.) AT/RT (infant, E) |
Vestibular schwannoma (E, involves internal auditory meatus) Meningioma (E with dural tail) |
| Lateral ventricle | Central neurocytoma (E) SEGA (tuberous sclerosis, E) Choroid plexus papilloma (E) Choroid plexus carcinoma (infant, E, large, invasive) |
Central neurocytoma (E) SEGA (tuberous sclerosis, E) Choroid plexus papilloma (E) Subependymoma (±E) Meningioma (E with dural tail) |
| Nerve root/Paraspinal | Neurofibroma (NF1, E) MPNST (NF1, E, necrotic) Melanotic schwannoma/malignant melanotic schwannian tumor (E, ±Carney complex) |
Schwannoma (E, dumbbell shape) Meningioma (E with dural tail) Secondary lymphoma (E) Neurofibroma (NF1, E) MPNST (E, necrotic) Melanotic schwannoma/Malignant melanotic schwannian tumor (E, ±Carney complex) |
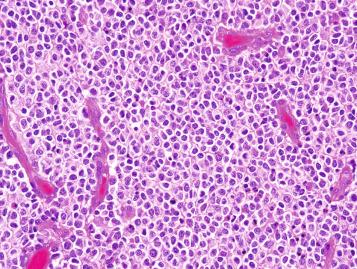
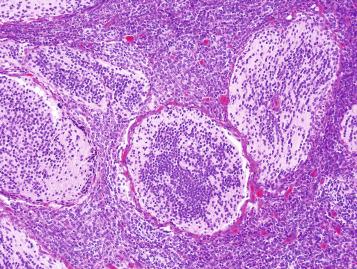
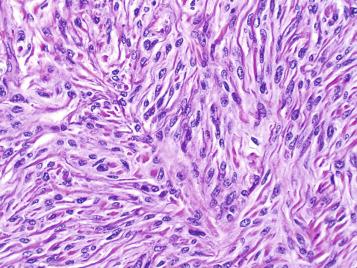
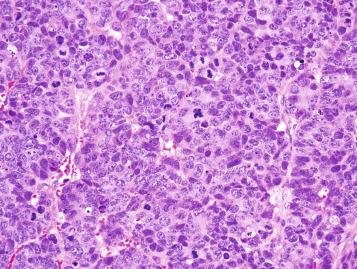
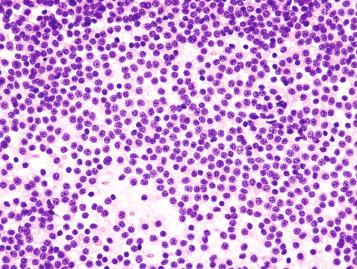
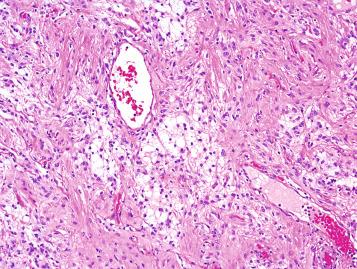
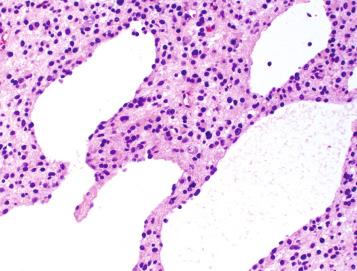
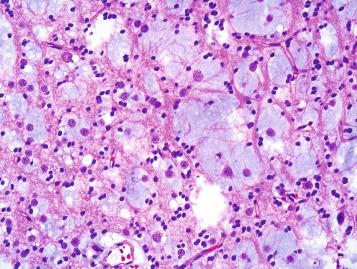
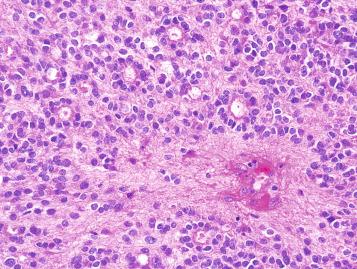
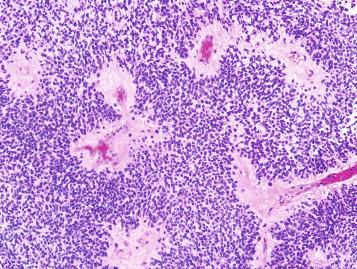
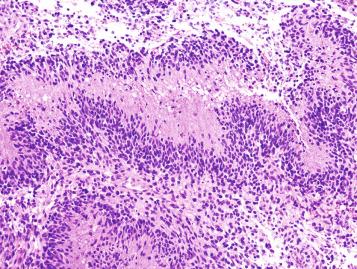
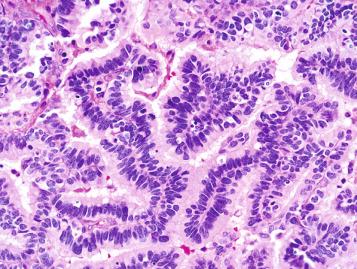
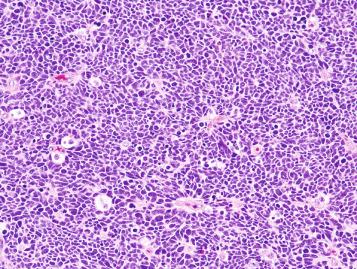
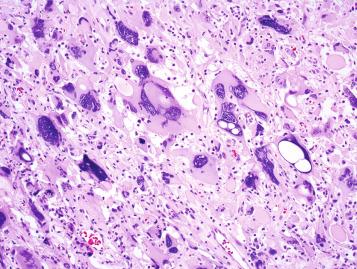
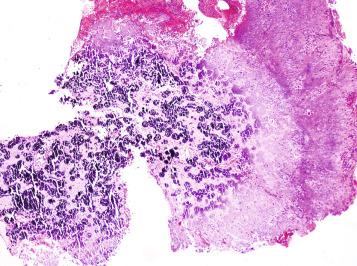
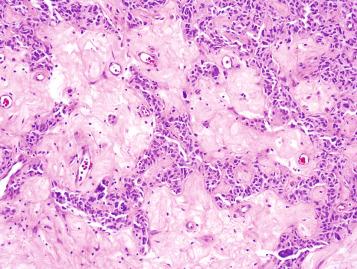
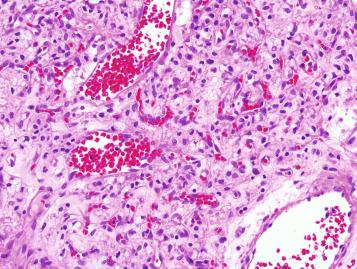
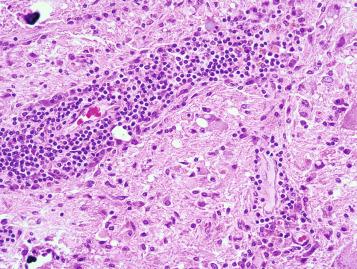
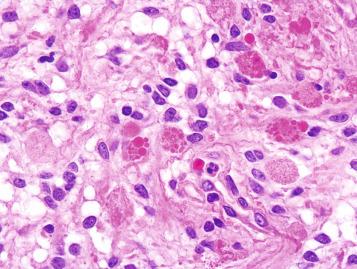
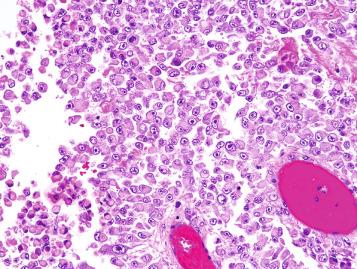
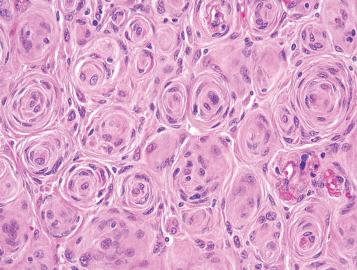
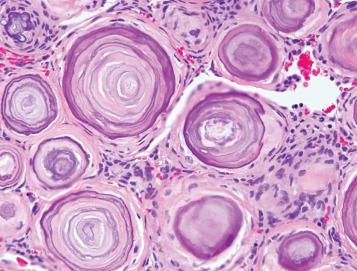
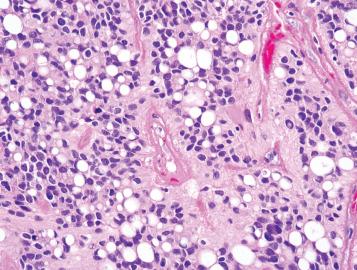
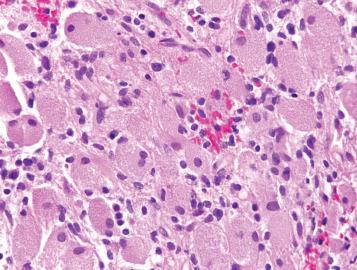
The next set of clues is naturally provided by classic histopathology. The 8 major patterns provided at the beginning of this textbook narrow the differential diagnosis considerably based purely on the overall low magnification appearance, and the subheadings of additional findings provide a useful diagnostic algorithm. When presented with a challenging biopsy, the pathologist can start with either the clinical- or morphology-based approach, but is encouraged to incorporate all available data before making a final diagnosis. In the vast majority of cases, the clinical, radiologic, and pathologic features are all consistent with one another; if not, the pathologist should very carefully reexamine the biopsy to ensure that all appropriate differentials have been considered and, if necessary, excluded or proven with ancillary studies. The use of common ancillary diagnostic techniques is briefly summarized in this chapter, with many more specific examples provided in the subsequent chapters on specific topics. As useful secondary algorithms, the major differential diagnosis based on an additional 24 minor histologic patterns is presented in Table 1.2 , with helpful clinicopathologic features summarized for 21 common differential diagnoses in Table 1.3 .
| Atypical Gliosis vs. | Diffuse Glioma (WHO Grade II) |
|
|
| Diffuse Astrocytoma vs. | Pilocytic Astrocytoma |
|
|
| Pleomorphic Xanthoastrocytoma vs. | Giant Cell Glioblastoma |
|
|
| Diffuse Glioma/Glioblastoma vs. | CNS Lymphoma |
|
|
| High-Grade Glioma or Lymphoma vs. | Demyelinating Disease |
|
|
| Glioblastoma vs. | Abscess |
|
|
| Glioblastoma vs. | Metastasis |
|
|
| Recurrence/Progression of Glioma vs. | Radiation Necrosis/Radiation Effects |
|
|
| Anaplastic Oligodendroglioma vs. | Small Cell Glioblastoma |
|
|
| Oligodendroglioma vs. | Diffuse Astrocytoma |
|
|
| Oligodendroglioma vs. | Dysembryoplastic Neuroepithelial Tumor |
|
|
| Oligodendroglioma vs. | Central/Extraventricular Neurocytoma |
|
|
| Oligodendroglioma vs. | Clear Cell Ependymoma |
|
|
| Ependymoma vs. | Diffuse Astrocytoma |
|
|
| Cellular Ependymoma vs. | Medulloblastoma/Embryonal Neoplasm |
|
|
| Medulloblastoma vs. | Atypical Teratoid/Rhabdoid Tumor |
|
|
| Medulloblastoma/Embryonal Neoplasm vs. | Glioblastoma |
|
|
| Meningioma vs. | Schwannoma |
|
|
| Meningioma vs. | SFT/HPC |
|
|
| Hemangioblastoma vs. | Metastatic Renal Cell Carcinoma |
|
|
| Hemangioblastoma vs. | Angiomatous Meningioma |
|
|
Although electron microscopy (EM) has historically been vital in defining a number of diagnostic entities, its everyday use in surgical neuropathology is generally labor intensive, time consuming, and expensive, with interpretation typically delayed by one to several weeks. For these reasons, EM has largely been supplanted by immunohistochemistry (IHC) and molecular pathology in most medical centers. Nevertheless, EM remains extremely valuable in specific scenarios; for instance, it is still the gold standard for proving ependymal differentiation in diagnostically challenging examples. As with lineage-specific immunostains, ultrastructural pathology primarily provides insight into various forms of cellular differentiation by visualizing organelles, other cytoplasmic constituents, and cell membrane structures (intermediate filaments, neurosecretory granules, synapses, pinocytotic vesicles, intercellular junctions, cilia, microvilli, basement membrane, etc.). Further examples of EM use in surgical neuropathology are provided in subsequent disease-specific chapters.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here